
Bay Area Lyme Happenings Series
UCSF has joined the Cohen Foundation’s nationwide Lyme Clinical Trials Network (CTN) for Lyme and tick-borne diseases. The new Lyme Clinical Trials Center (CTC) at UCSF was funded by a $1m grant from Bay Area Lyme Foundation and is led by Charles Chiu, MD, PhD, and Felicia Chow, MD, as co-principal investigators. As the West Coast ‘node’ in the network, UCSF’s new Lyme Clinical Trials Center will focus on interventional trials and diagnostic studies to improve diagnosis and treatment of Lyme disease.
In this presentation to patients with Lyme disease in Marin County just north of San Francisco, Dr. Chow explains how the CTC allows for a more diverse patient population to participate in Lyme clinical trials, which is critical for developing therapies that can help a wider range of patients. UCSF’s involvement also aims to help Bay Area Lyme raise awareness that Lyme disease is prevalent year-round in almost all California counties.
Dr. Chow discusses an upcoming trial at UCSF that will evaluate the use of transcranial direct current stimulation (tDCS) to improve cognitive symptoms in patients with chronic Lyme disease. Additionally, UCSF researchers are exploring the use of metagenomic sequencing and machine learning to develop more accurate diagnostic tests for Lyme and other tick-borne infections.
Note: This transcript of Dr. Chow’s presentation has been edited for length and clarity.
“I hope that through these clinical trials, we’ll be able to identify therapies that are helpful to patients and that, as a result, have an impact on clinically meaningful outcomes—from day-to-day function, quality of life, and all of those important measures that indicate that a treatment is successful.”
– Felicia Chow, MD
Jo Ellis: Welcome on behalf of Bay Area Lyme Foundation. My name is Jo Ellis, and I’m the director of education at Bay Area Lyme. Our mission is to make Lyme disease easy to diagnose and simple to cure. Firstly, I want to recognize that we have some MDs in the room. We are always grateful when we have clinicians’ support for our work on behalf of Lyme patients. I will now introduce Dr. Felicia Chow.
Dr. Felicia Chow is an associate professor of neurology and medicine at the University of California San Francisco, and she earned her medical degree from Johns Hopkins University School of Medicine. She completed her neurology residency at Brigham and Women’s Hospital and Massachusetts General Hospital where she served as chief resident. Following this, she pursued fellowship training in neuroinfectious diseases and HIV neurology at UCSF. Dr. Chow holds a master of advanced study degree in clinical research from UCSF. She’s a member of the American Academy of Neurology, the American Neurological Association, the Infectious Diseases Society of America, and the HIV Medicine Association. Bay Area Lyme Foundation is incredibly proud that due to the work, tireless efforts, and selfless giving from our donors, Bay Area Lyme was able to give UCSF a million dollars for the new Lyme Clinical Trials Center at UCSF. Please join me in welcoming Dr. Chow.

Felicia Chow: Thanks so much, Jo. This is not intended to be a lecture! I’m hoping that it can be more of a discussion. So there will be plenty of time for questions at the end, but if you have any questions as I’m talking, you’re also welcome to pipe up and ask your question in the moment.
I want to first talk about the Lyme Clinical Trials Network that UCSF is now a part of and what that means, and then talk about some of the people involved. I want to talk about neurological disease in Lyme disease and some of the patients that I’ve seen with neurologic involvement of Lyme disease. And then what I want to spend the bulk of the time talking about is some of the work UCSF is doing in the Clinical Trials Network as well as some upcoming trials that are in development—one of which is about to begin enrolling participants. We want to tell you all more about that and then talk about other trials and studies that are coming down the pike. And then I want to leave time for questions and to hear from you all.
UCSF is now part of the Lyme Clinical Trials Network. We are the first ‘node’ on the West Coast as part of this nationwide Clinical Trial Network. This network was started at Columbia University in New York City and funded by the Cohen Foundation. It is a network of different sites across the country—mostly on the East Coast except for us—focused on developing treatments and improving outcomes in people living with Lyme and other tick-borne diseases. And so what we’re doing at UCSF is thinking about interventional trials, but also diagnostic studies. Everyone in this room is well aware of the fact that one of the biggest challenges with Lyme disease is the fact that we don’t have great ways of diagnosing Lyme. So that’s a problem.
In addition to interventional trials and thinking about therapies, we’re also very interested in diagnostics and how we can develop better ways to identify people who have Lyme disease so that we can treat them appropriately. I’m a neurologist by training, but I do neuroinfectious diseases, which is this super sub-specialized area of neurology. There are not very many of us in the country—or the world—who focus on infections of the nervous system. But I see patients who have either an established neurologic infection affecting the brain, the spinal cord, muscles, nerves, or any part of the nervous system, or I see patients for whom there’s some suspicion of a neurologic infection. In that role, I have been involved in a lot of clinical trials related to neuroinfectious diseases, including in the realm of HIV-associated neurologic disease and in tuberculous meningitis.
Those are the two areas in which I’ve been involved in several trials including multi-site international trials. As someone with an interest in infectious diseases and with this background in clinical trials, I was always struck by how little there is in the world of Lyme in terms of treatments and then also in terms of active trials that are going on to address issues in terms of appropriate treatment and in terms of individuals who have persistent symptoms and who have chronic Lyme. On top of that, we also don’t have a whole lot of research going on to try to identify therapies that may be effective. And so this seemed like a great opportunity for us to be able to bring our expertise in doing clinical trials in the infectious diseases space.

And then we have Dr. Charles Chiu, who is the co-principal investigator of the network, and you can see him right here. Dr. Chiu has an infectious diseases background and is primarily in the lab. He runs our microbiology lab at UCSF and has his own research lab. He’s very interested in the diagnostic side of Lyme disease among other infections. I’ll talk more about the work that he’s doing, but it was a good way for us to come together with him on the laboratory diagnostic side and myself focused on clinical research and clinical trials to merge our expertise and do more research that can address the issue of people living with Lyme who are having persistent symptoms or who have not received an accurate and timely diagnosis.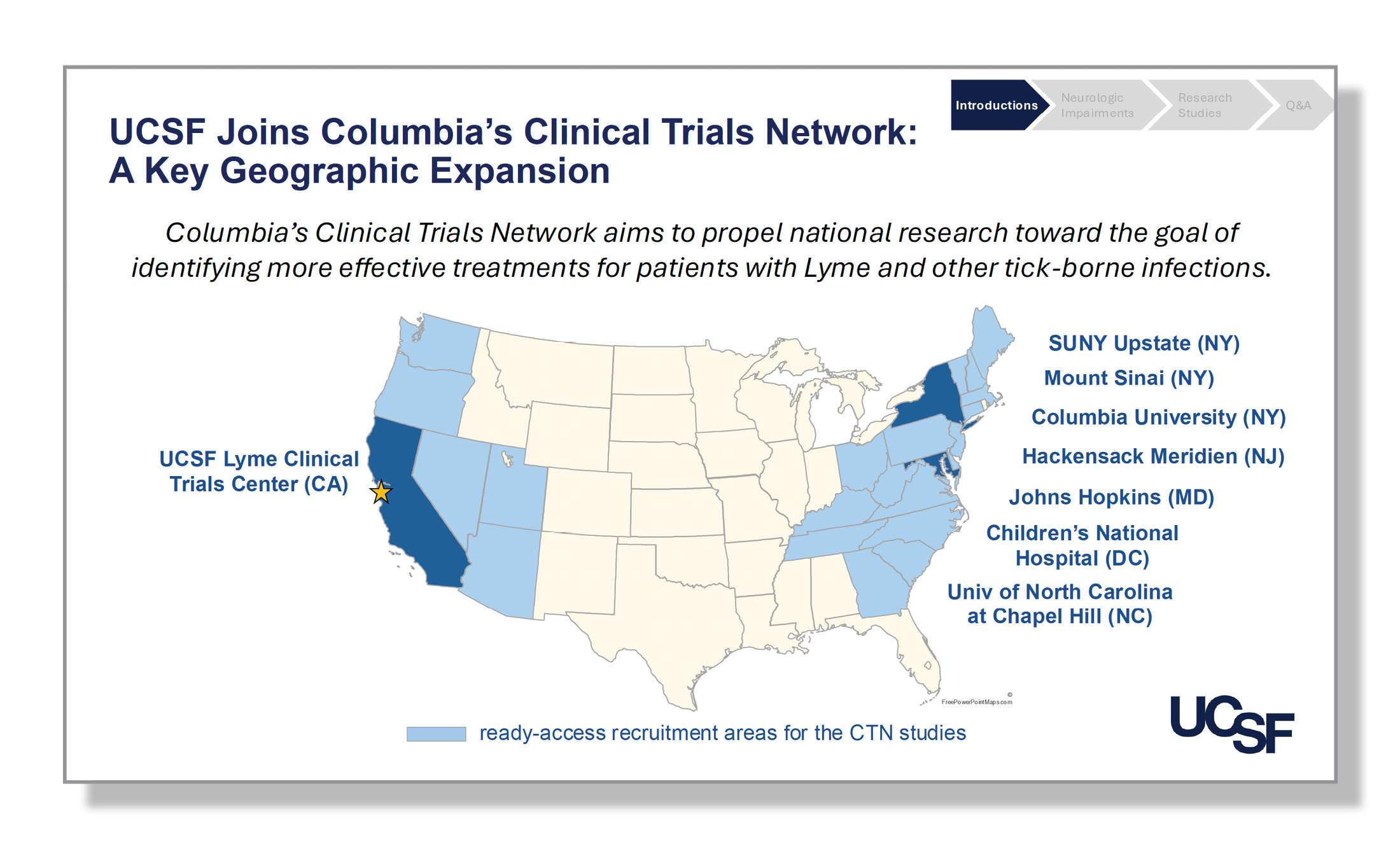
So as I mentioned, this is a national network of clinical trial sites and we’re thrilled to be able to have a presence on the West Coast. You can see the many other nodes that are involved in the network in the northeast, including New York and New Jersey, and then some in the Mid-Atlantic region down to North Carolina.
A few of these are newer and some were the initial nodes. For example, UNC I believe is a newer node and certainly Hackensack is as well. And then, as I mentioned, Columbia was one of the founding sites for the network. It’s been really exciting joining this network. We’re involved in frequent Zoom calls with the other nodes and have a chance to hear a little bit about the research that they’re doing, which is tremendously inspiring. I think one of the great things about including a West Coast site is the network will have access to a much more diverse population of potential participants who can be involved in these trials. As a result, findings that come from these studies will be more representative than if we were to only have people who are from the Northeast or a certain part of the country. That’s a big plus for us being involved in the network.
Here we are showing how the network is set up and you can see all of the different nodes that I mentioned. Again, Columbia is the coordinating center both administratively and in terms of a lot of the science that goes on. Columbia has taken a lead role in the work that’s being done, but now the other networks also are developing and starting up their studies and trials. Most of these are funded through the Cohen Foundation. At UCSF, we are unique because our funding comes from Bay Area Lyme, but I believe all, or at least most, of the other nodes, receive funding from the Cohen Foundation as one of their primary sources of funding for their trials.
This slide is intended to highlight some of the major pluses of having UCSF involved in the Clinical Trials Network. I think it’s great for us to be able to be a part of this larger network, but I think it’s also great for the network, great for the science, and great for the trials that are being done. One huge piece to this is that by being on the West Coast, we can expand access to these different trials to individuals like you who are here on the West Coast. In fact, since we have announced that we will be involved in these trials, we’ve already received emails from people up and down the West Coast who are interested in potentially participating.

So being able to expand that access is fantastic. And it’s not just the Bay Area. We’re hearing from people all over the West Coast. I think it’s nice to be able, as I mentioned, to work with all of these different sites across the country and to hear about the different work that’s being done. Dr. John Aucott at Johns Hopkins, for example, is doing a study using tetracycline. He has expertise in several different areas of Lyme, including Lyme arthritis for example. Dr. Brian Fallon is a psychiatrist. And Dr. Roberta DeBiasi, who’s in the network from Children’s National, is in pediatric infectious diseases.
The diversity of expertise that people bring to the network is amazing. I’ve learned a lot from discussions and brainstorming with the group. I have already mentioned what we can bring here on the West Coast in terms of enrolling a more diverse patient population into trials, which I think is critical. People still ask: ‘Is there even Lyme on the West Coast?’ I think because the prevalence of Lyme on the West Coast is not like it is in the highly endemic places in other parts of the country, we’re still making strides in terms of raising public awareness and helping people to understand that yes, absolutely, there is Lyme disease on the West Coast. Hopefully, the clinical trials network will help to do this, in addition to everything that is being done by Bay Area Lyme Foundation.

Finally, I hope that through these clinical trials we’ll be able to identify therapies that are helpful to patients and that, as a result, have an impact on clinically meaningful outcomes—from day-to-day function, quality of life, and all of those important measures that indicate that a treatment is successful. That is ultimately what we hope will come out of the Clinical Trial Network and being involved in it.
Lyme and Syphilis Negatively Impact the Brain at Any Stage of Infection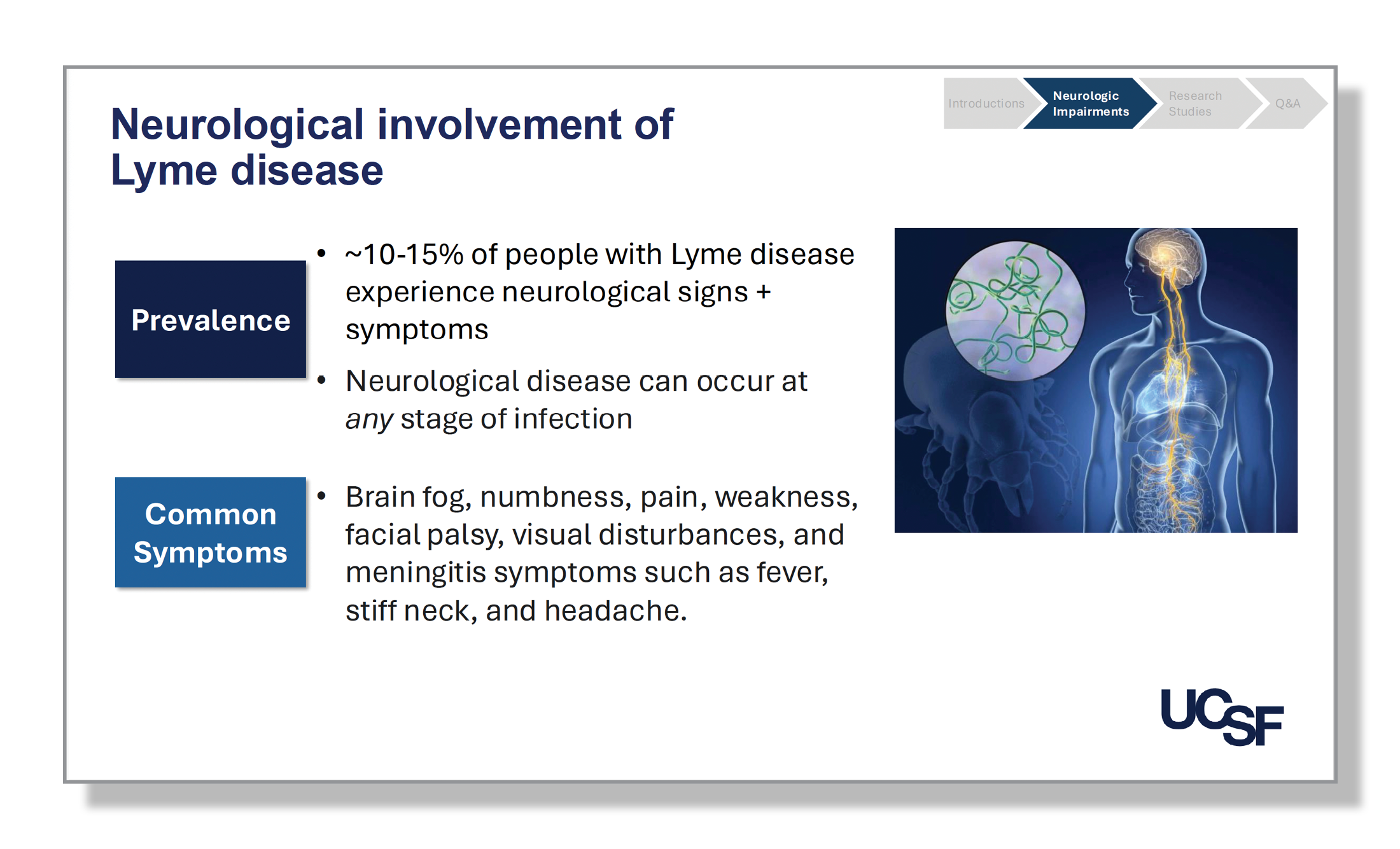
As I mentioned, I am a neurologist, and I see patients who have neurologic disease and neurologic signs and symptoms. I always point out when I’m talking to trainees that neurologic involvement of Lyme disease can occur at any stage of infection, just like in syphilis.
You can develop symptoms early in infection, what we call early or acute Lyme. And you can also have neurologic symptoms in a later-stage Lyme infection as well. An estimated 15% of people with Lyme may have neurologic signs and symptoms. I think that’s a challenging number to pinpoint for several different reasons, including the fact that we don’t have a ton of studies looking at the basic epidemiology of Lyme disease and of neurologic Lyme disease. On top of that, it always comes back to the challenge of diagnosis.
“I always point out when I’m talking to trainees that neurologic involvement of Lyme disease can occur at any stage of the infection, just like syphilis.”
– Felicia Chow, MD
It’s hard to know how often someone has neurologic involvement in an infection if we don’t always have great ways to diagnose the infection.
Cranial Nerve Involvement in Neurologic Lyme Disease
For neurologic Lyme disease, certain syndromes are commonly seen, including a meningitis picture. So that would include headache, neck stiffness, confusion, mental status changes, brain fog, and—oftentimes but not always—patients can have cranial nerve involvement. This means the nerves that come off the brain and control your eyes, ears, mouth, tongue, etc., can be affected if you have meningitis. For some people, you can have those cranial nerve abnormalities without meningitis. This would be, for example, someone who has experienced facial palsy. Having weakness on one side of your face is a common manifestation of neurologic Lyme and something that is easily recognizable. In addition to the cranial nerve that controls your facial movements, there are many other cranial nerves, 12 in total. For some cranial nerves, if they’re affected, it may be more subtle in terms of what you might develop. It may be numbness of the face, double vision, difficulty swallowing, slurred speech, and the list goes on and on, but several different cranial nerves can be affected.
How Autonomic Nervous System Issues are Affected by Lyme
What I’ve been seeing a lot of—and I have a couple of examples of these types of cases—is involvement of the nerves as they come off the spinal cord and lead into your arms and your legs and other parts of your body. For some people, this can present as numbness and tingling in your arms and legs or weakness in your arms and legs. It can also be the nerves even before they get all the way down to your extremities, but more in your torso and back.
It may present as extreme back pain or as sensory changes in the torso. And on top of that, because the nerves are affected, you can also get what we call autonomic nervous system issues, including urinary retention, constipation, dry mouth, symptoms that I think can be subtle—or maybe not subtle—but a lot more difficult to pinpoint and to understand what might be causing them compared with, ‘I’m not able to move one side of my body.’ When you can’t move one side of your body, that is something that physicians, neurologists, emergency room physicians, they see that and they’re like, ‘Oh, okay, something is going on either with the brain or the nerves that go to that part of the body.’ But when you have urinary retention or constipation, those symptoms may still be caused by a problem with the nerves, but some providers may be less likely to recognize them as neurologic issues.
“It’s hard to know how often someone has neurologic involvement in an infection if we don’t have great ways to diagnose the infection.”
– Felicia Chow, MD
In addition, some people may have more of what we call encephalitis or encephalopathy where it’s not so much the covering of the brain that is affected, which is what meningitis is, but rather the actual brain itself that can then lead to brain fog among several other signs and symptoms.
Neurologic Manifestations of Lyme Disease Run the Gamut
One of the reasons why I got interested in being involved in this Clinical Trials Network is that in the last 10 years or so, in the time that I’ve been seeing patients in my neuro-infectious diseases clinic, I was seeing more and more patients who either I was diagnosing with or who were coming to me already with a diagnosis of Lyme with neurologic manifestations. And it ran the gamut in terms of the types of neurologic syndromes that people had. This is just one example of someone who had several weeks of diffuse back pain.
It would occasionally radiate into the left chest and arms. Of course, he got this big cardiac workup thinking it was a heart attack. And in the context of getting that big cardiac workup, no one was thinking about a neurologic issue, and certainly Lyme was not on anyone’s radar. Then this person started to notice word-finding difficulty and brain fog. As part of the evaluation that we did, he had an MRI of his spine and it’s very difficult to make out in this lighting, but this is the spine here that we’re seeing sort of in cross-section this way, and all of the nerves coming off of the spine at the bottom and even the lower part of the spine itself were enhancing. This would imply that there was inflammation of the lower part of the spinal cord and of the nerves as they came off of the spinal cord.
And , I think hopefully you can make out all of these white dots here. This is the same spinal cord but in a cross-section this way, as if you’re taking someone’s spinal cord and cutting it this way. All of these little white spots here shouldn’t be there. In a ‘normal’ MRI of the spine, you wouldn’t see that. But that is essentially where each of those nerves as they came out of the spine were inflamed. We did a bunch of other testing including Lyme testing and it was positive. This is someone who lived in the Bay Area and had not traveled to Humboldt or Marin or other areas more known to have Lyme. I think because of that, there was a delay in the diagnosis, but fortunately, the diagnosis was made and he received treatment.
Audience Member: Can you see similar scans of the brain where it shows up material like that?
Felicia Chow: Yes, absolutely. Great question. Somehow all of the cases I am talking about today, none of them are actually of the brain, all spinal cord. But yes, so I mentioned before that you can get meningitis and you can get cranial nerve involvement, both of which typically happen early in infection. If you get a brain MRI at that time, you can see the same enhancement that I showed here in the covering of the spinal cord and the spinal nerves but rather of the cranial nerves as they come out of the brain. So you can get cranial nerve enhancement and you can also get enhancement just of the covering of the brain itself, or the meninges. Both of those findings are relatively common, again, in early neurologic Lyme. I think the issue is that for a lot of patients, by the time they get their brain MRI, it may be weeks, or months after their symptoms, and so the enhancement perhaps is already resolved at that point.
“In my neuro-infectious diseases clinic, I was seeing more and more patients who either I was diagnosing with or who were coming to me already with a diagnosis of Lyme with neurologic manifestations.”
– Felicia Chow, MD
Audience Member: So they can still be experiencing neurological issues without showing on the MRI.
Felicia Chow: Yes, absolutely.
Numbness, Tingling, Weakness, and Pain – Evidence of Inflammation on MRI
Okay, so this slide is sort of similar. I just wanted to point out someone who had terrible shoulder and arm pain followed by numbness, tingling, and weakness in the hand. It was the right hand. Then—same thing—after some time they became increasingly confused. And so again, Lyme was so far off people’s radars, that wasn’t something that was being considered at all. But she ended up having an MRI of the brachial plexus, which is essentially when all the nerves come out of your spinal cord and they go down into your arm, there’s a big collection of the nerves here in the shoulder before they fan out into your arm. And that’s called the brachial plexus. This person had, in terms of their symptoms, a very classic syndrome of a brachial plexus problem.
And indeed, when she finally had her brachial plexus image, I know it’s a little hard to make out, but you can trust me that there is enhancement of the brachial plexus and I think you can appreciate the difference between the two sides. And everything on MRIs is flipped. So this is the right side, and this is her left side. And so here on the right brachial plexus, you can appreciate that it’s generally brighter compared with this side. When the radiologists read this, they felt that this side was also potentially a little bit abnormal, but not to the degree that this side was. So, a similar story. It took a long time for her to be diagnosed. Fortunately, when she was finally diagnosed and treated she had a good response to treatment, although she still had some residual numbness, tingling, and weakness in that hand after being treated.
“People still ask, ‘Is there even Lyme on the West Coast?’ We’re still making strides in terms of raising public awareness and helping people to understand that yes, absolutely, there is Lyme disease on the West Coast.”
– Felicia Chow, MD

And the same thing with a bunch of other cases, someone with bifacial weakness and meningitis, someone that I saw not too long ago with relapsing fever, urinary retention, constipation, somnolence, and someone else who had high fever, extreme fatigue, and brain fog. Each of them had neuroborreliosis. The first was Lyme, and then the second two were Borrelia miyamotoi, another Borrelia infection that is similar in some ways to Lyme—at least in terms of some of the neurologic manifestations—but different obviously in that it’s not Borrelia burgdorferi.
This slide is the textbook diagram that some of you have perhaps seen before. I made the point before that neurologic disease can happen at any point in infection.
I think the biggest issue with the bullseye rash is that it doesn’t occur in a large percentage of people or because it doesn’t itch and it’s not painful, it may be missed in some people. I think the other thing—and this is something that I talk a lot with our trainees about—is that the textbook images we have of the bullseye rash are of people who are fair-skinned. I should have included an example of that. So that classic bullseye rash that all the people who’ve been trained in medical school are looking for is going to not look like that in someone who has dark skin.
I think the other big thing, of course, is what we’ve already mentioned quite a bit, diagnostics are a big problem. That is something that Charles Chiu, as I mentioned, is interested in. And I have a couple of slides coming up that talk a little bit about some of the really exciting work that his group is doing to try to improve the diagnosis of Lyme, both acute Lyme and, because so many people may present later on, in terms of chronic disease. Charles is also interested in not just diagnostics, but also thinking about how we can use various tests to monitor response to treatment.
Upcoming Clinical Trial: Prefrontal Cortex Stimulation Targets Cognitive Decline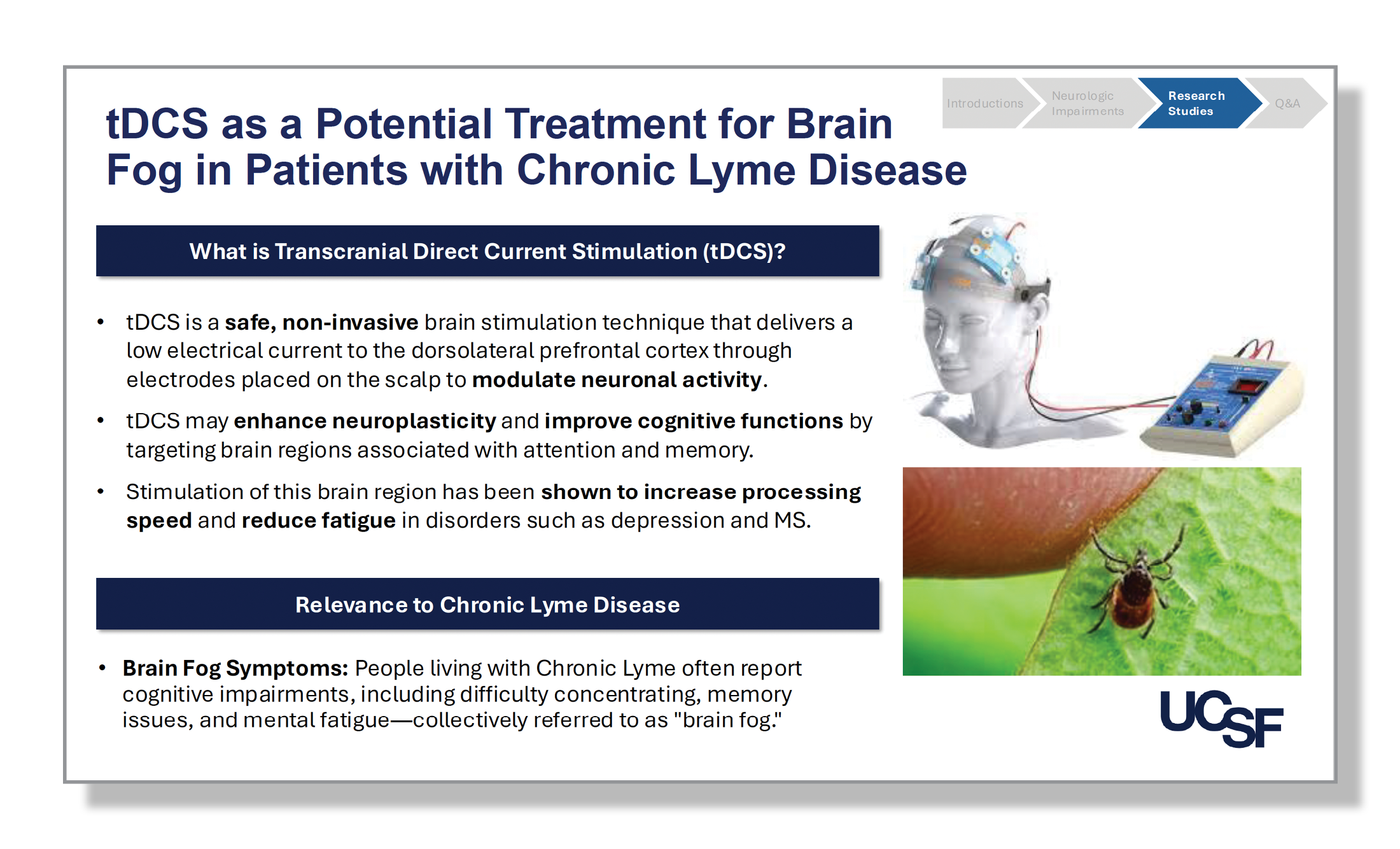
One of the things that I was excited to come and chat with you all about today is some of the trials that we’re actively doing. The clinical trial that we are right now working on with Columbia—it’s a two-site trial headed up by Columbia, and it’ll also occur at UCSF—is this study here. This is a study that will use Transcranial Direct Current Stimulation (tDCS) as a potential treatment for people who are living with chronic Lyme and have brain fog. The study will target people who have ongoing cognitive symptoms, which we know is a very common persistent symptom for a lot of people with Lyme.
What exactly are we doing? So first, what is tDCS? Transcranial Direct Current Stimulation—you can see a picture of it here. This is a noninvasive procedure. Everything goes on top of the head as you can see in this photo. It’s a safe technique that essentially does exactly what it sounds: it delivers low electrical current to parts of the brain, and it targets the dorsal prefrontal cortex, which is roughly here through these electrodes that are placed on the scalp. The idea is that sending this current through the scalp can enhance neuroplasticity and how the brain is responding to injury from Lyme. It can improve cognitive function by specifically targeting areas, including the prefrontal cortex and the dorsolateral prefrontal cortex, that we know are associated with some forms of cognitive impairment that are common in people living with Lyme. This includes issues with attention and memory.
The reason why Columbia decided to look at tDCS is because it’s been shown in a couple of studies of other types of neurologic illnesses to have benefits, including MS and depression. It has been shown specifically to lead to improvement in terms of fatigue as well as improving processing speed—two major symptoms that a lot of people living with chronic Lyme may have. I think that is why Columbia was interested in using tDCS as a potential therapy for people with chronic Lyme.
Audience Member: Is it one treatment or a series of treatments?
Felicia Chow: Great question. Most of the actual trial will take place in your homes. You get the device, you take it home with you, and some training goes along in terms of how to place it, and the things that need to be done. But again, most of it is in your home where you’re doing the treatments. The study runs for 12 weeks and there are four in-person visits to UCSF. As part of those visits, there are a bunch of study procedures that are done, including blood draws, some clinical questionnaires, and then a cognitive assessment as you might imagine. Then there is training in terms of how to use the tDCS device and then also online cognitive training as well. The study, of course, has a set list of inclusion and exclusion criteria.
Inclusion and Exclusion Criteria for tDCS Trial
We have highlighted a couple here. There is an age cutoff, so it’s 18 to 65 years of age and you have to have been diagnosed with Lyme disease. But given what we’ve talked about and the challenges of diagnosis of Lyme that is pretty flexible in terms of that definition. We’re looking for individuals who may have definite, probable, or possible Lyme, and I use those terms knowing they come with a lot of potentially loaded meanings. I think this is all to say that you don’t have to meet CDC criteria to be enrolled in the study. In addition to that, of course, because we’re looking at the impact on cognitive symptoms, you have to have current cognitive symptoms. To qualify for the study, we’re doing cognitive testing and you have to score within a certain range to qualify for the study.
“You don’t have to meet CDC criteria to be enrolled in the study.”
– Felicia Chow, MD
Audience Member: And it has to be during an active infection?
Felicia Chow: I think the critical thing here is that we’re looking for individuals who have been treated already with antibiotics, at least two courses, and are still having brain fog and cognitive symptoms. Beyond that, to be eligible you need to meet the diagnostic criteria. And then I think the other thing, of course, is at least during the 12 weeks that you’re on treatment and in the study, you have to be willing to not start any new treatments for Lyme because that obviously could interfere with what we may or may not see in terms of the tDCS. So that’s the shortlist. There is a longer list of eligibility criteria, and if you’re interested of course in learning more, the website is here in terms of our Clinical Trials Network. And this is our clinical research coordinator’s email. Please feel free to reach out, even if you think you might be interested, but don’t think you’re going to qualify. Send us an email anyway because we’d love to chat and learn more about you. Even if you’re not eligible for this study, we can certainly put you on a list if you’d be interested in hearing about future studies.
Audience Member: Is the purpose of the 65 age cutoff because other sources of brain fog may be present?
Felicia Chow: The short answer is yes. That is often why we have age cutoffs for trials. I think that especially now with better diagnostics becoming available for Alzheimer’s and other disorders, I’m hoping that in terms of study design for all clinical trials, we will rethink having this age cutoff because I don’t think it’s always necessary. But yes, that is exactly why. Thank you.
Audience Member: What’s the threshold for the official diagnosis of Lyme disease?
Felicia Chow: It’s a pretty long document that the Clinical Trials Network has developed and is following in terms of the Western blot and the number of bands that must be present. There are many different ways that you can meet the diagnostic criteria.
Audience Member: Have you already started this?
Felicia Chow: No. We are in the process of getting the Institutional Review Board (IRB) approval, and I think based on how long things can take with the IRB, I would say hopefully early 2025.
Audience Member: Thank you so much for this talk. First of all, it’s super interesting and we are very, very grateful for anybody doing any Lyme research in the world. Do you happen to have a grasp on where the spirochetes are located within the brain? Is the purpose of having it in the dorsal lateral zone solely for memory, or is there a communication happening between where the
Felicia Chow: Yes, that’s a great question. The selection of the dorsolateral prefrontal cortex is based purely on the types of cognitive impairments that have been most commonly described in people with Lyme, including impaired processing speed and memory impairment. Additionally, in a lot of the other studies, and to be very honest, there haven’t been many, but of the studies that have been done, a lot of them have also targeted this area.
Audience Member: With the images you showed of the spinal cord, what kind of inflammation is occurring? Do we know what biomarker it is that’s expanding?
Felicia Chow: That’s also a great question. I’ll talk a little bit about some of the blood-based biomarkers that we’ve been looking at in terms of Lyme diagnostics, but we don’t know specifically what it is in the spinal fluid that is causing the inflammation we’re seeing in these MRIs. It’s probably a combination of different inflammatory markers. The contrast enhancement shows us that there is some breakdown of the blood-central nervous system barrier and that there’s some inflammation present.
Audience Member: I wondered if the tDCS would also affect the orbital frontal cortex, so maybe it would help this area.
Networks in the Brain and How Phenotypes Impact Brain Fog
Felicia Chow: Yes. Absolutely. The orbitofrontal cortex is near the areas we are targeting, all of which are part of the prefrontal cortex. So they’re all closely linked. I think that another thing about this research focused on the brain is that it’s all about networks and the connections between the different areas of the brain. And certainly, if you have brain fog versus some other neurologic symptom, these different phenotypes could be related to different parts of the brain.
Audience Member: I think in maybe looking at it because you’re saying, ‘Well, where does the Lyme go?’ My understanding is that at least one way is that it comes from the blood, it goes into the choroid plexus, the little capillaries where the blood is filtered into the clear cerebral spinal fluid and the little rooms of the brain, the ventricles, and then it penetrates through the ventricular area into the brain parenchyma. Maybe there are other routes, but that’s my understanding of how it gets into the brain.
Felicia Chow: That would be a pretty typical sort of route for a lot of the infections and pathogens that we see in the brain that are crossing the blood-brain barrier through as you said, the choroid plexus and then ultimately causing meningitis or encephalitis. Other questions?
Audience Member: So for someone with a diagnosis of Alzheimer’s located in that area, especially someone who’s only 50 years old and who was a horse person/equestrian, wouldn’t it be reasonable to get tested for Lyme? She went to the best doctors at UCLA. I can’t convince this person to get tested.
Felicia Chow: Absolutely. Yes. I think it just speaks to the fact that there are many different ways in which Lyme can manifest, including with cognitive impairment. If someone is being diagnosed with Alzheimer’s at age 50, that would be quite atypical, so we will look for alternative diagnoses. And I think in addition to looking for alternative diagnoses, we also are looking for alternative, treatable diagnoses, and Lyme would be one to consider. I would encourage people to think broadly in situations like that.
Metagenomic and Next-Generation Sequencing in Dr. Charles Chiu’s Lab
I want to talk a little bit about some of the laboratory testing work that Charles Chiu and his group are doing.
Some of you all maybe have heard about metagenomic next-generation sequencing. This is a relatively new technology that has changed our approach to the diagnosis of infectious diseases. The general idea is that with metagenomic next-generation sequencing, you take a specimen, whatever you’re looking at, it’s either spinal fluid, blood, or biopsy tissue from somewhere, and you extract and sequence all of the genetic material from the specimen.
You can take out all of the human sequences because as you can imagine in a specimen of blood or spinal fluid, there’s a lot of genetic material that comes from the host, the patient, and that’s what they’re showing here. But if you remove all of the human sequences, so you can tell what’s human and what’s not, if you remove all of those sequences, then you can identify in the remaining genetic material potential pathogens that may be causing an infection. And so that’s the idea: you are taking everything that you find in that clinical sample and sequencing it, and that may help you to identify an infection.
This is something that is being done at UCSF, and we can do it on spinal fluid and, in a research capacity right now, on different types of tissue specimens. And it can also be done on blood. What Charles is interested in in terms of Lyme diagnostics is instead of removing the human sequences, he’s interested in looking specifically at these sequences in the host (patient), to see whether or not that will help in the diagnosis of Lyme. Because the idea is that when you have an infection, your body has a response to that infection.
And so when you have a response, you’re making inflammatory markers, you’re making proteins, all the different things to fight that infection. So, for example, if you take a bunch of patients who have Lyme, sequence all of their genetic material from a blood specimen, and see what’s different between someone who has Lyme versus someone who doesn’t, you could identify unique signatures to help diagnose someone with Lyme. Instead of going after the pathogen, we’re going after how the body is responding to the pathogen. That’s the idea behind a lot of the work that Charles is doing in terms of diagnostics. This is a couple of slides to show some of that.
Determining What Biomarkers are Upregulated in the Blood of Lyme Patients
The first thing they’re doing is some comparisons between people who have chronic Lyme, long COVID, and chronic fatigue and taking blood samples from these different participants. And essentially they are sequencing all of the genetic material from their blood samples. Then they are looking to see what biomarkers, what proteins, and what cytokines are upregulated in these different types of infections to see whether or not there’s a certain pattern that emerges for the different types of infections. By doing that, they have been able to identify biomarkers that are upregulated in people with chronic Lyme, and then see how they may be distinct from some of these other types of infections.

In addition to identifying individual biomarkers, they’re also interested in using machine learning, AI, to not just look for individual biomarkers for these different infections but to see groupings or clusters of biomarkers that are associated with infections.
Charles’s goal is to be able to identify a cluster of biomarkers that can help to diagnose someone with Lyme in the same way that we currently use ELISA, Western blot, and other diagnostic tests. This would be a much more nuanced and advanced way to be able to see individuals who have this unique signature versus just looking for an individual protein or small group of proteins.
Because right now that is what an ELISA or Western Blot does. Those tests are looking for at most a couple of specific proteins at a time. By doing this sequencing of all of the genetic material and then clustering with machine learning, we can look at thousands of proteins, even more, to understand which groupings of these different markers may be abnormal in some with Lyme disease.
This slide is showing a similar study, instead of chronic Lyme, long-term COVID, and chronic fatigue, they were looking at people with a bunch of other types of infections, including flu, babesiosis, anaplasmosis, some people with COVID, and then some asymptomatic individuals as well, or people without any sort of infection.
They were able to identify unique signatures in people who had Lyme versus people who did not. And then similarly, in terms of some of the other infections—we just happened to pull the Babesia versus no Babesia cases—using machine learning techniques they were able to identify super accurate ways to classify people with and without Lyme and with and without babesiosis, with more than 90% accuracy. By refining this technique further, hopefully, this can be used for diagnosis in addition to what we currently use.
“Using machine learning techniques they were able to identify super accurate ways to classify people with and without Lyme and with and without babesiosis, with more than 90% accuracy.”
– Felicia Chow, MD
Audience Member: Can we draw from any of the research on syphilis for how we approach live disease with spirochetes? Or is that not a correlating disease?
Felicia Chow: As I mentioned earlier, clinically there are similarities between the two types of infections. Syphilis is one of the infections where metagenomic sequencing has not been particularly helpful in making diagnoses. And that’s because in the spinal fluid, for example, of someone with neurosyphilis, we don’t usually use PCR testing to identify genetic material for syphilis. Instead, we rely on antibody testing to diagnose syphilis. There’s just not a high burden of spirochetes that can be identified in spinal fluid.
Lyme seems to be similar. That’s why it is not high yield to send a Lyme PCR test to look for genetic material in the CSF of someone with neurologic Lyme disease. I’m not aware of us having any samples from people with syphilis to see how similar or different genetic signatures may be in someone with Lyme versus syphilis. But it’s a good question and I can ask Charles, he may have some samples that we could do and compare because I think it would be interesting.
Clinical Trial for Rapamycin to Treat Persistent Lyme Symptoms
I have just one more slide about other clinical studies that we are talking to collaborators about, and excited that hopefully, we’ll be able to roll these out. There is one that I wanted to highlight using low-dose rapamycin for treating persistent symptoms that are seen in long COVID and Lyme. With long COVID there has been a lot of renewed interest in terms of people who have chronic symptoms after an infection. One of the treatments that is being looked at is rapamycin, an mTOR inhibitor. It’s something that we use clinically, in people who’ve had transplants and you want to suppress their immune system. You can give rapamycin so that they don’t reject the transplant they’ve received.
So it has an impact on the immune system, but at lower doses than what’s used for transplant patients, it has other effects that may be beneficial for long COVID and also for Lyme. At lower doses than what we give to transplant patients, it’s been shown to have anti-inflammatory and anti-angiogenic benefits, meaning it inhibits the formation of new blood vessels. And that’s another important concept that may help in terms of some of the different persistent symptoms after infections, like long COVID. It actually also has some antifungal properties. I think when it was first developed, it was developed as an antifungal agent. So, there are a lot of intriguing properties of rapamycin that have made people want to look at it as a potential therapeutic agent.
The last one I’ll mention is that it has a lot of anti-aging effects too. That is of interest as there’s overlap in terms of what we’re seeing may be activated in people with persistent symptoms after Lyme and aging pathways, including the mTOR pathway. In a large study in Europe, they found a genetic variant that was associated with a higher risk of Lyme disease and mapped to the mTOR pathway. Because rapamycin inhibits the mTOR pathway, which may be upregulated in some patients with Lyme disease, there is general excitement about rapamycin being a potentially effective therapeutic agent for chronic Lyme. We have a collaboration with investigators at the Mount Sinai Clinical Trials Network node who are already planning a study of rapamycin for long COVID. Once they have that trial up and running, we’re hoping we’ll be able to roll out a similar trial for people living with chronic Lyme. More to come on that hopefully soon.
I want to acknowledge several different people who’ve been involved in terms of the start of the Clinical Trial Center at UCSF, first and foremost, the Bay Area Lyme Foundation and also the Lyme Disease Biobank, and Liz Horn who is the principal investigator for the Biobank. The team at UCSF, many of whom I’ve mentioned, and at Columbia. A lot of our partners there, especially on this tDCS study, have been leading the charge. They’re the ones who designed the study. They have IRB approval and should be starting up fairly soon. And so we’ve been working very closely with them and hoping that we’ll be able to start up shortly as well.
Audience Member: There are so many people getting Lyme disease every year, and those are just the people who know they have Lyme disease. Why isn’t it taught in medical school? I mean, there’s a half a million people every year diagnosed with Lyme disease. Why don’t doctors understand it?
Felicia Chow: I’m trying to remember back to medical school in terms of the specific teaching that was done. I think speaks to the fact that the textbook descriptions and presentations of Lyme can be different than what people experience. And I think we need more research to be done so that the textbook descriptions are accurate and include the more varied presentations that we see with Lyme that you are familiar with.
The Challenge with Current Diagnostic Tests
Audience Member: I think most of us have diagnosed ourselves, we figured it out ourselves or from a friend or somebody. It doesn’t ever seem to come from a doctor.
Felicia Chow: And I think that is, in part, because of challenges with diagnostics. It’s a problem for sure.
Audience Member: So this is an official question and you can give me an official answer. There is a lot of testing. A lot of laboratories give diagnostic tests using different methods in terms of testing science and technology and the definitiveness of testing results when how much reliability one could give on a certain testing result of certain companies using different methods. And which method do you think, among all the methods existing right now perhaps has the higher validity and reliability than other methods? That’s one question. Secondly, if a persistently negative outcome or negative result is of the testing process, does that prove conclusively that the patient or the test has no Lyme? Because there are different criteria for measuring Lyme CDC is a criteria alternative. There’s the CDC, another alternative. Different doctors have different criteria for even coming to that conclusion. So there is some kind of chaos or some ambiguities in those testing arenas. So how would you recommend if unofficially we go around in the realm of testing and which method would you think right now has a superiority to other methods?
“I think the biggest issue is that the bullseye rash doesn’t occur in a large percentage of people…also the textbook images we have of the bullseye rash are of people who are fair-skinned.”
– Felicia Chow, MD
Felicia Chow: Yeah, so it’s a great question. I’ll take your second question first in terms of if you have negative testing over and over again, and whether that means that you can definitively rule out Lyme. I think it depends on what you mean by negative testing. I think it also depends on where in the course of your illness you may be. One thing I often get worried about, and I’ve seen this quite a bit in my clinic, is people who come to me who feel that they have Lyme despite the fact that their testing has been negative. The patient is focused on Lyme and not necessarily thinking about other potential diagnoses, and some providers are focused on this being another patient who is convinced they have Lyme and also not thinking about other potential diagnoses. I think the most important thing when seeing a patient coming in with whatever the list of symptoms may be, is to make sure that we’re thinking broadly about all of the potential processes that may be explaining their symptoms, whether it be an infection or something else, and if it is an infection, what are all of the different possible infections that it can be?
I think one thing that I do worry about, and I have seen this, is that because our diagnostics are imperfect, and it can be hard to diagnose Lyme, people may say, I have a negative test, but I still think I have Lyme and that’s what I’m going to focus on. And in fact, I saw someone not too long ago who it turned out had something completely unrelated to Lyme. Their diagnosis was delayed because they were convinced they had Lyme, and they’d been going to physicians who were supporting the idea that it was a Lyme infection, and it turned out not to be.
I just want to be sure that we don’t swing the opposite way where we are only thinking that something is Lyme, when in fact the testing is a true negative, and it is, in fact, something else. It is not uncommon for me to see patients who have an immunoblot with several positive bands but not enough bands to meet CDC criteria. In those situations, other data can help to inform a diagnosis of probable Lyme, including most importantly that they have a clinical syndrome that fits with neurologic Lyme, like the syndromes I mentioned earlier. Then when we do get, say, a spinal tap, in the spinal fluid we obtain additional information to support a diagnosis of neurologic Lyme. So there is quite a bit of nuance to the diagnostics, including whether you had an immunoblot after your ELISA was potentially negative? And whether you received any antibiotics with activity against Lyme before the ELISA was done? And if you did get the immunoblot, if you didn’t meet CDC criteria, was someone still thinking about interpreting your results in the context of your clinical presentation and saying it could still be Lyme even though you may not have had 5 or more bands? Then in the right clinical context, did they do additional testing to help look into it further? For me, additional testing is often spinal fluid, which can aid in making the diagnosis.
Audience Member: So in that case, again, it’s a witch hunt. It is kind of like a maze that you have to go through unless it’s typical like tuberculosis or other bacterial infections where it’s black and white.
Felicia Chow: Not for neurotuberculosis. Sure, there are some infections where the diagnosis may be more clear-cut, but definitely not for tuberculosis.
Audience Member: But for other infections, there’s a black and white test, for example, COVID, if whatever the test value or not, it’s black and white, you have it or you don’t have it. With Lyme it is almost like detective work. Well, you have it, but maybe not have it, but let’s try this. It’s all about ambiguity. And so at this point, I mean it seems like a spinal tap is the only final definitive test.
Felicia Chow: No, I don’t mean to imply that either because the other problem with spinal fluid is, and this is all specific to neurologic Lyme if you have central nervous system signs and symptoms early in infection, your spinal fluid may be, should typically be, abnormal. But if you are years out from acute infection, it may not be abnormal. The other issue is that a lot of people have what we call peripheral neurologic Lyme, so it may be more nerves out here, in the extremities for example. In that situation, the spinal fluid may be normal. Actually by no means is spinal fluid definitive testing. I was just using that as an example for certain situations.
But in terms of your first question and all the different companies who offer testing, that’s tricky too. The problem is that there are a lot of companies out there that are doing different types of testing. Some testing is validated, but a lot of it is not. I think the really important thing, with iGeneX testing or whatever lab it may be, is that you’re working with a physician who will help to interpret the results of the testing in the context of the entire picture.
If I have someone who’s coming to me and their signs and symptoms are not typical of neurologic Lyme, that’s important to know in addition to what their spinal fluid shows, what their lab testing shows, et cetera. I think it’s about not necessarily saying, okay, they don’t meet the five band criteria or they don’t meet whatever criteria, so that’s it. It’s definitely not Lyme. That’s a cognitive error. On top of that, there are other considerations, like cross-reactivity and thinking about whether or not there may be another type of related Borrelia infection that may be going on. For example, if a Lyme test is only partially positive because they actually have a different type of Borrelia or tick-borne infection.
Audience Member: There are like 60 or 12 different kinds of it.
Felicia Chow: There are different types of Borrelia and that’s happened to some patients I’ve seen where they don’t meet diagnostic criteria for Lyme, but they ended up having another Borrelia infection, like Borrelia miyamotoi. I think it ultimately comes down to being sure you’re working with someone who can help to make sense of test results in the context of the entire clinical picture.
Audience Member: There are thousands of treatments that we have probably all tried. How did this study identify the tDCS to study?
Felicia Chow: That study is being led by Columbia. I think that they have been scouring the literature to learn from what we know about other diseases. Because in MS, in depression, et cetera, where some of those same areas of the brain that may be affected have been shown to potentially benefit from tDCS, that was something they were particularly interested in. Columbia is doing a couple of other studies, but this just happened to be the one that at the time that we were coming on board, they were looking for additional sites that could help enroll. That’s how we got involved. But I think with a lot of the other potential therapeutics that we’ll be looking at—like rapamycin—the idea is to be sure that there’s a strong rationale before moving forward. And, with funding et cetera, most funders aren’t going to fund a trial unless there is a strong reason to think that intervention may be effective. For rapamycin for example, it’s because of the link with the mTOR pathway identified in the cohort of people with Lyme in Europe that piqued our interest, in addition to what we know about rapamycin and its potential effects on inflammation, aging, et cetera.
Audience Member: With Bay Area Lyme’s funding of Timothy Haystead‘s work, does that make them any more likely to run his future trials? It seems like he said, seeing is believing and what he’s doing with PET scans to detect reservoirs in the body will end up really what moves the needle as far as believing chronic Lyme. I believe you’re part of the LINK study as well is what Duke is doing with finding viral reservoirs with PET scans. It seems like UCSF would be uniquely able to also do that and all those requirements. And yeah, I was wondering if you guys are looking at some of those unique imaging offerings as well as secondly some of these overlappings with COVID and bonding components that lead to brain fog?
Felicia Chow: I can’t speak to the funding aspect of things in terms of what Bay Area Lyme may be likely to fund, but I think your bigger question about reservoirs is one that certainly is of tremendous interest in a lot of different infectious diseases. You mentioned COVID-19, I think even in the HIV world, there’s a huge push now to cure HIV and all of the questions swirling around the ability to do that come down to the reservoir. So places in the body where HIV or whatever fill-in-the-blank pathogen may be persisting and may be particularly difficult to get to. And I think of those different reservoirs, the first priority is understanding where they may be. And then secondly, when you have identified the different reservoirs, how you’re going to make sure that the treatments you have are getting to those different places is critical.
Of those reservoirs, we know the brain is a privileged space, and while pathogens can infect the brain, it can be extremely difficult to get treatments into that privileged space. That’s a huge challenge, a recurring theme in neuro-infectious diseases, how to get treatments across the blood-brain barrier. There’s a reason why it exists, but you have to be able to penetrate that barrier for treatments to work.
Jo Ellis: I want to thank Dr. Felicia Chow for her fascinating presentation, and all of you for coming out tonight. Thank you, everyone, on behalf of Bay Area Lyme Foundation.
NOTE: Dr. Chow’s neuro-infectious disease clinic sees patients with untreated or recently treated neurologic Lyme disease. This clinic does not currently see chronic Lyme or tick-borne disease patients. The Lyme Clinical Trials center profiled in this blog plans to initiate clinical trials to test different interventions for Lyme disease, but will not be able to provide comprehensive care for chronic Lyme patients. Participants in UCSF clinical trials will need to maintain care through existing providers. Biography: Felicia Chow is an Associate Professor of Neurology and Medicine at the University of California, San Francisco. Dr. Chow earned her medical degree from Johns Hopkins University School of Medicine. She completed her neurology residency at Brigham and Women’s Hospital and Massachusetts General Hospital, where she served as chief resident. Following this, she pursued fellowship training in neuro-infectious diseases and HIV neurology at UCSF. Dr. Chow holds a Master of Advanced Study degree in clinical research from UCSF. She is a member of the American Academy of Neurology, the American Neurological Association, the Infectious Diseases Society of America, and the HIV Medicine Association. This blog is part of our BAL Happenings Series. Bay Area Lyme Foundation provides reliable, fact-based information so that prevention and the importance of early treatment are common knowledge. If you wish to register your interest in being part of future UCSF clinical trials, please complete the form on our website here. If you require a copy of this article in a bigger typeface and/or double-spaced layout, please contact us here. You may read an earlier blog based on an interview with Dr. Chow here. For more information about Bay Area Lyme, including our research and prevention programs, go to www.bayarealyme.org. Photos courtesy University of California San Francisco.