
A rash associated with early Lyme disease, called erythema migrans (EM), has long been considered the hallmark sign of acute infection with Borrelia burgdorferi, the primary cause of Lyme disease in the United States. However, many people with Lyme disease do not have an observed or reported EM, and the classic “bullseye” (ring-within-a-ring) rash that many people associate with Lyme is relatively uncommon.
The Centers for Disease Control and Prevention (CDC) defines EM for surveillance purposes as an expanding round rash, often with partial central clearing (ring-like), measuring at least 5 cm (about 2 inches) in diameter. It should be emphasized that this definition is used to track cases nationally for public health surveillance; however, it does not mean a skin lesion must be at least 5 cm for a physician to diagnose EM clinically.
While multiple scientific journal articles, as well as the CDC, report that up to 80% of cases may exhibit the EM, a comprehensive review of peer-reviewed published studies and surveillance reports shows that EM rates can be substantially lower and can vary by region, study design, and the patient population being evaluated. In many datasets, around 50% or fewer may have an observed or reported EM. For example, population-based studies by public health departments in three states found the proportion of Lyme disease patients with EM was 51% (Delaware in 2000-2004 study), 43% (Maine in 2010 study), and 33% (California, 2019 Annual Report).
When the rash does occur, it’s usually within 3–30 days after infection. However, there are reports, including data from the Lyme Disease Biobank, that show EMs can appear even earlier.
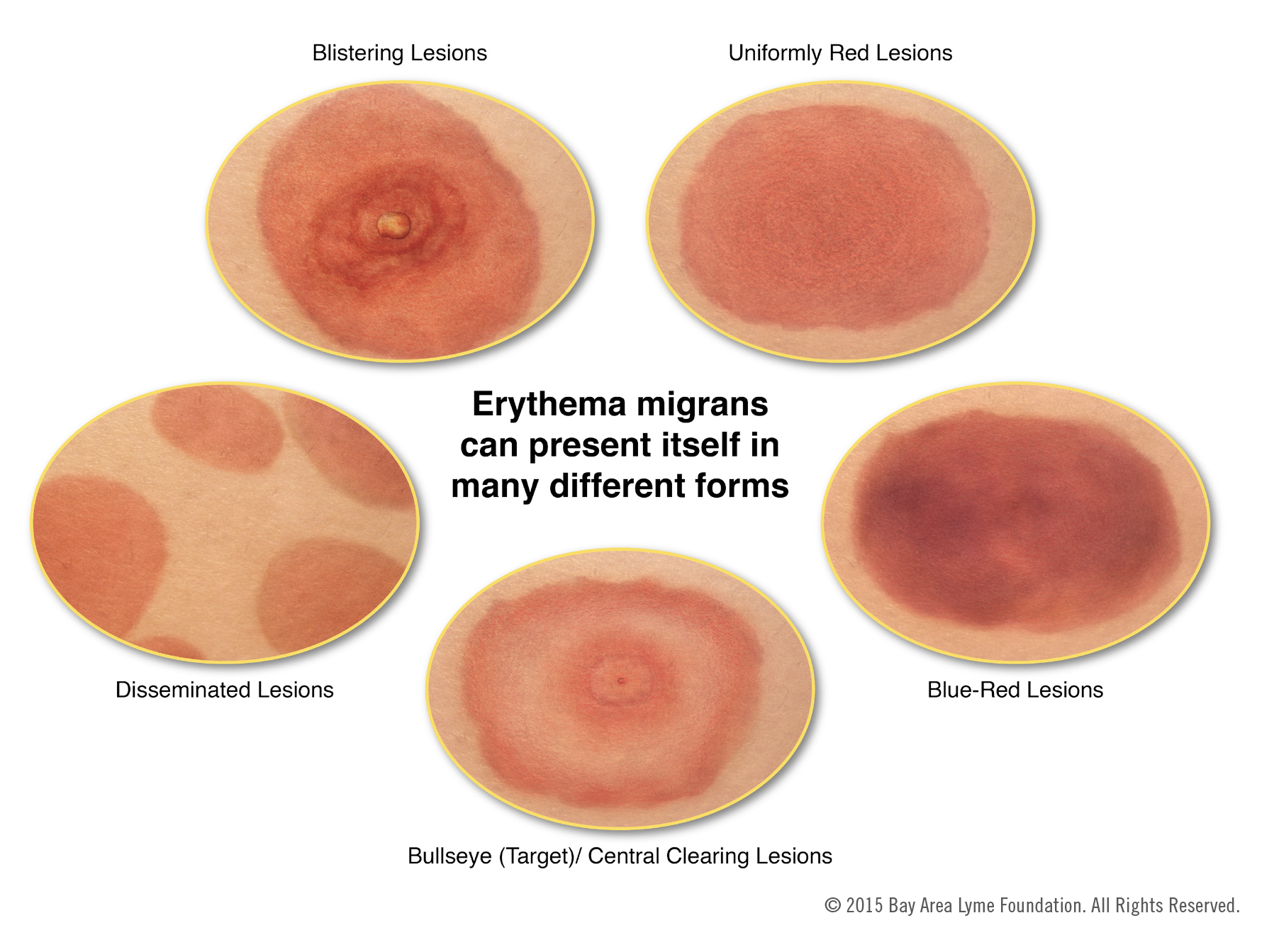
When present, the rash can take many forms. It is usually red, flat, round, and in some cases will develop central clearing as it expands (hence the name “bullseye rash,” which refers to an annular, or ring-like, appearance), but, more commonly, it is homogeneously red throughout. In a 2022 study reviewing suspected rash images from patients with early acute Lyme disease enrolled in Lyme Disease Biobank, approximately half were homogenous throughout, and just 6% showed the classic bullseye pattern.
Occasionally, the rash can develop a bluish cast like a bruise or take irregular, elongated, or angular shapes. It is usually warm to the touch and may have a raised bump (induration) in the center. It can be associated with a feeling of burning or, less commonly, mild pain or itching. The rash may not be observed, may pass unnoticed, or may not be recalled. The rash can be accompanied by other symptoms, such as fatigue, fever, headache, and muscle or joint pain.
What to do if you have a rash
If you have a rash, the best thing is to document it: take a picture next to a ruler so you can determine the size. This can be very helpful to a healthcare provider in evaluating the rash. You can also draw a ring around the contours or mark the edges to see if it expands over time.
If you see multiple EM rashes (these can form close to the original rash or in other places), this indicates a disseminated infection. Again, take a picture of the rashes and contact your healthcare provider immediately. Disseminated infection means the infection has circulated via the bloodstream and could be present in other body organs, for example, the brain, heart, joints, or eyes. Immediate treatment with antibiotics is important to help prevent more severe complications of infection, like Lyme neuroborreliosis or Lyme carditis.
The chart below illustrates several of the forms these rashes might take.
There are many symptoms of Lyme disease, and it is critical that you are alert to all of them. See Lyme Disease Symptoms for more information.
Don’t Be Fooled
Lyme disease is often referred to as the great imitator because so many of its symptoms resemble those of other diseases. Without a telltale skin rash, it can be very hard to diagnose Lyme disease. Many people never recall being bitten.
Below is a list of some of the diseases that many people have initially been diagnosed with, only to receive a Lyme diagnosis later:
- Cellulitis: bacterial infection involving the skin and underlying soft tissues, which presents with an erythematous rash that can appear similar to a homogeneous erythema migrans rash
- Arthritis: typically manifests as joint pain, swelling, redness, heat, and limitation of movement
- Juvenile idiopathic arthritis: a childhood disease that causes joint inflammation and swelling
- Fibromyalgia: especially widespread muscle and soft tissue pain
- Chronic fatigue syndrome: the most prominent and defining symptom is severe and debilitating fatigue, especially post-exertional fatigue
- Multiple sclerosis: leading to problems with muscle control and strength, vision, balance, sensation, and mental functioning
- Lupus: may affect joints (pain, swelling), skin, kidneys, brain, and other organs
If you suspect Lyme, even if you do not recall being bitten, discuss the situation and symptoms with your doctor.
Image courtesy of Emily M. Eng