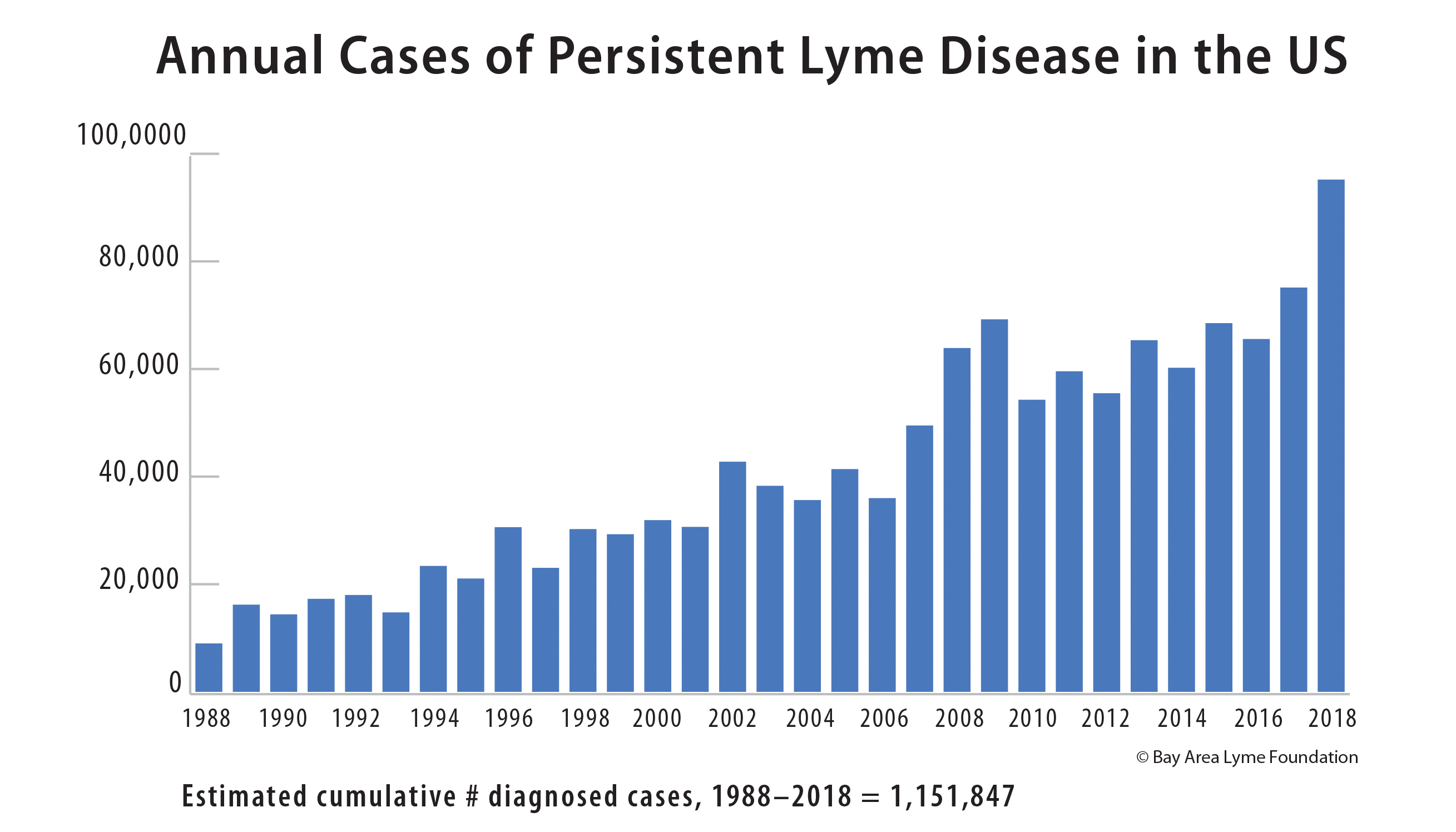
Up to two million Americans may be suffering from the impact of persistent Lyme disease. Research has shown that up to 30% of Lyme patients have ongoing symptoms, which in some cases can be severe and debilitating. Many clinicians and scientists believe that the persistence of bacteria is the cause of these lingering symptoms, so while the CDC calls this “post-treatment Lyme disease syndrome,” we believe it is more accurate to use the term “persistent Lyme disease” (PLD). The term PLD supports the scientific belief that the disease can live on beyond treatment. The studies below demonstrate the existence of persistent infection, giving validity to the terms “persistent” and “chronic. The studies below, many funded by Bay Area Lyme, demonstrate the existence of persistent infection, giving validity to the term persistent Lyme.
Studies That Support the Persistence of Lyme Disease
Lyme disease and the pursuit of a clinical cure
Heather Adkison and Monica E. Embers*
Robust B Cell Responses Predict Rapid Resolution of Lyme Disease
Blum, Lisa K.; Adamska, Julia Z; Martin, Dale S.; Rebman, Alison W.; Elliott, Serra E.; Cao, Richard R. L.; Embers, Monica E.; Aucott, John N.; Soloski, Mark J.; Robinson, William H. Frontiers in Immunology. 2018; 9: 1634.
This paper, funded by Bay Area Lyme Foundation, demonstrates that a robust immune response is associated with more rapid resolution of Lyme disease, and patients who reported persistent symptoms exhibited lower levels of immune response at the initial visit as compared with those that returned to health.
Variable manifestations, diverse seroreactivity and post-treatment persistence in non-human primates exposed to Borrelia burgdorferi by tick feeding
Embers, Monica E; Hasenkampf, Nicole R; Jacobs, Mary B.; Tardo, Amanda C.; Doyle-Meyers, Lara A.; Philipp, Mario T.; Hodzic, Emir. PLOS One 2017.
This paper, funded by Bay Area Lyme Foundation, demonstrated that living B. burgdorferi spirochetes were found in ticks that fed upon the primates and in multiple organs after treatment with 28 days of oral doxycycline. The results also indicated that the immune response to the bacteria varied widely in both treated and untreated subjects.
Late Disseminated Lyme Disease: Associated Pathology and Spirochete Persistence Posttreatment in Rhesus Macaques.
Crossland, Nicholas; Alvarez, Xavier; Embers, Monica. American Journal of Pathology 2017.
“Rare morphologically intact spirochetes were observed in the brains of two treated rhesus macaques, the heart of one treated rhesus macaque, and adjacent to a peripheral nerve of an untreated animal.” Treatment consisted of 5 mg/kg doxycycline administered orally twice daily for 28 days.
B. burgdorferi persisted in patients with EM despite antibiotic treatment
Hunfeld KP, Ruzic-Sabljic E, Norris DE, Kraiczy P, and Strle F. In vitro susceptibility testing of Borrelia burgdorferi sensu lato isolates cultured from patients with erythema migrans before and after antimicrobial chemotherapy. Antimicro Agents Chemother 2005; 49: 1294-1301.
“Borrelial isolates obtained from five patients with erythema migrans (EM) before the start of antibiotic therapy and again after the conclusion of treatment were investigated. Four of five patients had positive skin biopsy cultures that tested positive after treatment with 14 days oral antibiotics and the fifth was treated with both oral and IV antibiotics. The study substantiates borrelial persistence in some EM patients at the site of the infectious lesion despite antibiotic treatment over a reasonable time period. Borrelial persistence, however, was not caused by increasing MICs or minimal borreliacidal concentrations in these isolates. Therefore, resistance mechanisms other than acquired resistance to antimicrobial agents should be considered in patients with Lyme Borreliosis resistant to treatment.”
Lyme Disease spirochete may persist actively or latently in the central nervous or musculoskeletal system for years
Nocton JJ, Bloom BJ, Rutledge BJ, Persing DH, Logigian EL, Schmid CH, Steere AC. Detection of Borrelia burgdorferi DNA by polymerase chain reaction in cerebrospinal fluid from patients with Lyme Neuroborreliosis. Journal of Infectious Diseases 1996; 174: 623-627. https://pubmed.ncbi.nlm.nih.gov/8769624/
This paper demonstrates that PCR positivity for OspA, the very specific surface protein for B. burgdorferi, exists even in the case of antibiotic-treated patients. In this case series, there is a correlation between duration of IV antibiotic treatment and PCR positivity rate—i.e., the longer someone is on IV antibiotics (but not oral) the less likely they are to have a positive PCR. 12/25 patients treated for less than 28 days (oral, IM or IV) still PCR positive. 2/22 patients treated for greater than 28 days (up to 150 days) still PCR positive—10% failure rate. The two patients that tested positive in this group were treated with 2 months oral and then only 2 weeks IV antibiotics. Note that CSF more likely to be positive than serum, especially in neuroborreliosis. However, 2/12 IV antibiotic-treated patients were still PCR positive for OspA protein. None of the 42 controls’ CSF samples tested PCR positive, so chance of sample contamination causing PCR positive tests extremely low. Authors stated: “This provides the best evidence to date that the Lyme disease spirochete may persist actively or latently in the nervous system for years. This prolonged disease course, with long periods of active and latent infection, is reminiscent of tertiary neurosyphillis”
Nocton JJ, Dressler F, Rutledge BJ, Rys PN, Persing DH, Steere AC. Detection of Borrelia burgdorferi DNA by polymerase chain reaction in synovial fluid from patients with Lyme arthritis. N Eng J Med 1994; 330: 229-234. https://www.ncbi.nlm.nih.gov/pubmed/8272083
This study evaluated synovial fluid from almost a hundred patients over 17 years at two different labs. Synovial fluid (SF) samples from both pre and post treatment specimens were collected, using four different primer sets for PCR detection. Three primer sets targeted OspA plasmid DNA and one target set targeted DNA of ribosomal RNA. No control samples tested positive using this methodology. 12/12 SF samples were positive after a short course (<1month) of oral antibiotics, with sample taken and tested from 2 months to 4 years post treatment. 7/19 patients treated with either longer courses of oral antibiotics (median 37 days) or IV antibiotics (median 14 days, range to 20 days) remained PCR positive for Borrelia OspA. Patients with negative PCR results tended to have been treated longer than those with negative PCR responses, although the difference was not statistically significant. Of 10 patients with “chronic Lyme arthritis” despite multiple courses of antibiotic therapy, 3 remained PCR positive for OspA.
B. burgdorferi persistence may exist even when serum is negative for antibodies
Preac-Mursic V, Weber K, Pfister HW, Wilske B, Gross B, Baumann A, Prokop J. Survival of Borrelia burgdorferi in antibiotically treated patients with Lyme borreliosis. Infection 1989; 17(6): 355-359.
Antibiotic therapy may abrogate the antibody response to the infection as shown in our patients. B. burgdorferi may persist as shown by positive culture in MKP-medium; patients may have subclinical or clinical disease without diagnostic antibody titers to B. burgdorferi. We conclude that early stage of the disease as well as chronic Lyme disease with persistence of B. burgdorferi after antibiotic therapy cannot be excluded when the serum is negative for antibodies against B. burgdorferi. Presented here are 5 cases treated with either IV ceftriaxone or penicillin for 10-14 days, and 1 case treated with 10 days oral doxycycline. All cases were borrelia culture positive from 1 month to 7.5 months after treatment.
Borreliae were found in the bladder despite antibiotic treatment
Chancellor M, McGinnis P, Kilholma P, Hirsch I: Urinary dysfunction in Lyme disease; Journal of Urology. 1993 Jan;149(1):26-30.
Seven patients with confirmed neuroborreliosis and resulting urologic dysfunction, who often required catheterization, were enrolled in this study. In one patient who had rapidly progressing neurological symptoms and subsequently fell into a coma, spirochetes were visualized using two different methods in a bladder wall biopsy, despite a prior 3-week course of IV ceftriaxone and Borrelia antigens were also found in urine. One case also showed, despite neuroborreliosis and an erythema migrans, persistently presented with negative antibodies to borrelia in the blood using common testing regimens, and blood-based antibodies remained negative, despite the fact that antibody titers in the CSF were positive.
Case study of patient with Lyme who died of ARDS with no signs of any other pathogens, despite doxycycline, penicillin treatment
Kirsch M, Ruben FL, Steere AC, Duray PH, Norden CW and Winkelstein A: Fatal adult respiratory distress syndrome in a patient with Lyme disease. JAMA 1988, 259:2737-9.
Woman with EM rash was treated with 14-day course of oral tetracycline—during regimen, she was ELISA positive for both IgM and IgG antibodies to B. burgdorferi. Her symptoms persisted. One month later, she was admitted to the hospital with highly abnormal liver function tests, rashes and joint complaints, and given 10-day course of IV penicillin. Her symptoms, including liver function, improved, and she was discharged 9 days later. She was readmitted 5 days later, and due to with elevated LFTs, she was retreated with IV penicillin, then high dose prednisone for lung infiltrates and inflammation. However, her rash worsened and she developed edema. She was readmitted to hospital with elevated temperature, pulse rate and respirations, joint swelling, and immunoblotting (Western blot) highly positive for IgG antibodies, with high level of bilateral central infiltrates in lungs. Open lung biopsy revealed severe, acute, diffuse alveolar damage compatible with ARDS, but no evidence of tumor, infection, or vasculitis. She also tested negative for EBV, CMV, Hepatitis A, B, Legionella, and Trichinella. She continued to worsen, while blood cultures for borrelia showed no growth. Patient died of ARDS but autopsy found cardiomegaly with borderline right ventricular hypertrophy, fatty liver, and necrosis of kidneys. Lymph nodes showed transformed lymphocytic response and spirochetes compatible with B. burgdorferi when Dieterle silver stain used. Lungs negative for influenza, parainfluenza, RSV, adenovirus and coxsackievirus.
Case study shows PCR positive and microscopic evidence of persistent Lyme infection in central nervous system after months of IV and oral antibiotic therapy.
Gadila SKG, Rosoklija G, Swork AJ, Fallon BA and Embers ME (2021): Case study with Validation Among Autopsy Specimens. Front.Neurol. 12:628045.
Patient with EM and mild neurologic symptoms treated with 10 days doxycycline. Two years later develops sleeping issues, 4 years later develops cognitive issues such as processing speed, mental tracking, and word finding in addition to other issues. Brain scans show atrophy and hyperintensities plus decreased perfusion. Treatment with IV ceftriaxone for 8 weeks led to 60% symptom improvement, but symptoms regressed on switching to oral amoxicillin and then minocycline. Clinically diagnosed with Alzheimers, then Lewy Body Dementia. Autopsy tissue showed PCR positivity in spinal cord and amygdala tissue, and intact spirochetes were visualized in spinal cord.
Case study demonstrated positive Borrelia PCR test following 5 courses of antibiotics
Lawrence C1, Lipton RB, Lowy FD, Coyle PK: Seronegative Chronic Relapsing Neuroborreliosis: European Neurology. 1995;35(2):113-7.
Patient with neuroborreliosis was given 5 courses of oral and/or IV antibiotics. After last three courses, PCR of CSF confirmed persistent Bb DNA of OspA, which is highly specific for B. burgdorferi. Patient remained PCR positive (tested in two labs) after 5 courses of antibiotics. In addition, this paper demonstrates that a patient with late stage disease, in this case PCR positive Lyme neuroborreliosis, remained antibody negative in the blood using two-tiered test algorithm. In this case, seronegativity of late stage disease was shown to be the result of immune-antigen complexes, where antibodies bind antigen in the blood stream such that the antibodies are not available to bind to the diagnostic antigen. This was confirmed by disassociating the serum antigen from the antibody and retesting, when a positive result was obtained with the unbound serum antibody. Importantly, this finding counters the assertion by health authorities that two-tiered serological testing is 100% accurate in late disseminated Lyme disease.
Case study demonstrates potential role of inappropriate immune response and location of B. burgdorferi in chronic Lyme
Häupl T, Hahn G, Rittig M, Krause A, Schoerner C, Schönherr U, Kalden JR, Burmester GR. Persistence of Borrelia burgdorferi in ligamentous tissue from a patient with chronic Lyme borreliosis. Arthritis Rheum. 1993 Nov;36(11):1621-6
The patient whose case is presented herein had relapsing Lyme borreliosis, with choroiditis, arthritis, carditis, and tendinitis. Patient was diagnosed subsequent to a 2 month prior tick attachment with progressive disturbance of central vision and multifocual choroiditis and given oral doxycycline for 6 weeks. Patients symptoms worsened, developed carditis and arthritis, and IV ceftriaxone administered for 14 days. Carditis and arthritis subsided, but visual disturbances reoccurred, but CSF negative for usual markers of borrelia infection. Antibiotic therapy resumed with 3 different oral antibiotics, but patient developed trigger finger and surgery was required. Patient permanently lost 70% of right eye vision. Biopsy of finger ligament was culture positive for borrelia, and isolate was additionally confirmed by PCR. “In conclusion, an inappropriate immune response as well as the evasion of B. burgdorferi into specific sites that are only slightly accessible to antibiotics and immunologic attack, may be mechanisms that lead to chronic infection with B. burgdorferi.“
B. burgdorferi persists in mice despite treatment with various classes of antibiotics
Barthold SW, Hodzic E, Imai DM, Feng S, Yang X, and Luft BJ. Ineffectiveness of tigecycline against persistent Borrelia burgdorferi. Antimicrob Agents Chemother 2010; 54(2): 643-651.
Antibiotics are likely to kill most B. burgdorferi organisms, but the immune system is needed to fully eliminate the remaining spirochetes. However, B. burgdorferi has evolved to persistently infect fully immunocompetent mammalian host. The current study examined the efficacy of tigecycline, a new first-in-class glycylcycline, which is the most potent antibiotic against B. burgdorferi on a weight basis in vitro. Tigecycline is a structural analog of minocycline that avoids tetracycline resistance mediated by inhibition of bacterial efflux pumps and ribosomal protection. However, using both low and high doses of tigecycline, essentially similar findings of persistence of noncultivable, infectious spirochetes were found, as previously shown with ceftriaxone and doxycycline. Thus, the phenomenon of B. burgdorferi persistence appears to be universal among these various classes of antibiotics.
Following antibiotic treatment, mice remained infected with nondividing but infectious spirochetes, particularly when antibiotic treatment was commenced during the chronic stage of infection
Hodzic E, Feng S, Holden K, Freet KJ, Barthold SW (2008) Persistence of Borrelia burgdorferi following antibiotic treatment in mice. Antimicrob Agents Chemother 52: 1728-1736. PMCID2346637
The effectiveness of antibiotic treatment was examined in a mouse model of Lyme borreliosis. Mice were treated with ceftriaxone or saline solution for 1 month, commencing during the early (3 weeks) or chronic (4 months) stages of infection with Borrelia burgdorferi. Tissues from mice were tested for infection by culture, PCR, xenodiagnosis, and transplantation of allografts at 1 and 3 months after completion of treatment. In addition, tissues were examined for the presence of spirochetes by immunohistochemistry. In contrast to saline solution-treated mice, mice treated with antibiotic were consistently culture negative, but tissues from some of the mice remained PCR positive, and spirochetes could be visualized in collagen-rich tissues. Furthermore, when some of the antibiotic-treated mice were fed on by Ixodes scapularis ticks (xenodiagnosis), spirochetes were acquired by the ticks, as determined based upon PCR results, and ticks from those cohorts transmitted spirochetes to naïve SCID mice, which became PCR positive but culture negative. Results indicated that following antibiotic treatment, mice remained infected with nondividing but infectious spirochetes, particularly when antibiotic treatment was commenced during the chronic stage of infection.
While B. burgdorferi are susceptible to antibiotics in vitro, these bacteria can persist in a host animal model similar to humans
Embers ME, SW Barthold, JT Borda, et al. Persistence of Borrelia burgdorferi in rhesus macaques following antibiotic treatment of disseminated infection. PLoS ONE 2012;7(1): e29914.
These results demonstrate that B. burgdorferi can withstand antibiotic treatment, administered post-dissemination, in a primate host. Though B. burgdorferi is not known to possess resistance mechanisms and is susceptible to the standard antibiotics (doxycycline, ceftriaxone) in vitro, it appears to become tolerant post-dissemination in the primate host. This finding raises important questions about the pathogenicity of antibiotic-tolerant persisters and whether or not they can contribute to symptoms post-treatment…. In some cases, patients who have been treated for Lyme disease experience persistent symptoms. The assertion that further antibiotic treatment is warranted in these cases is a matter of contention and considerable debate. Our results indicate that disseminated spirochetes of two different B. burgdorferi strains can persist in the primate host following high dose, or longlasting antibiotic therapy… Our studies do however offer proof of the principle that intact spirochetes can persist in an incidental host comparable to humans, following antibiotic therapy. Note: subsequent to this study, many labs have published that B. burgdorferi is not eradicated in vitro by standard antibiotics, including doxycycline, amoxicillin, and ceftriaxone, unless a cocktail of three antimicrobials are co-administered.
The Lyme disease spirochete was detected up to three weeks after the initiation of antibiotics treatment with strains of co-infecting B. burgdorferi
Mosel MR, Carolan HE, Rebman AW, et al. Molecular testing of serial blood specimens from patients with early Lyme disease during treatment reveals changing co-infection with mixtures of Borrelia burgdorferi genotypes. Antimicrobial Agents and Chemotherapy 2019.
Borrelia burgdorferi is the etiological agent of Lyme disease. In the current study, we used direct detection PCR and electrospray ionization mass spectrometry to monitor and genotype B. burgdorferi from serially collected whole blood specimens from clinically diagnosed early Lyme disease patients before and during 21 days of antibiotic therapy. B. burgdorferi was detected up to three weeks after the initiation of antibiotic treatment with ratios of co-infecting B. burgdorferi genotypes changing over time.
Congressional Testimony
Persisting viable but non-cultivable B. burgdorferi is now a convincing phenomenon
Congressional testimony of Stephen Barthold, DVM, PhD, Distinguished Professor Emeritus, UC Davis 2012.
“Persisting viable but non-cultivable B. burgdorferi is now a convincing phenomenon based upon a number of animal-based (mouse, dog and primate) studies using a number of different antibiotics, and the significance of continued infection indeed needs to be better understood. It is time to recognize that Lyme disease is not a simple bacterial infection.”
A special thank you to Raphael Stricker, MD, Union Square Medical Associates, and past President and current Board Member of the International Lyme and Associated Diseases Society (ILADS), and Lorraine Johnson, JD, MBA, CEO, Lymedisease.org for their investigations into the persistence of Lyme bacteria. The references for their studies laid the groundwork for this list.