
Ticktective Podcast Transcript
In this interview, author/filmmaker, Kris Newby, explains the murky history behind the US government’s involvement with Lyme disease and continued efforts to hide how the military’s bioweapons programs caused the spread of tick-borne pathogens. She explains how alliances between pharmaceutical companies, insurance companies, university-based research teams, and the government led to inaccurate testing and denials of care, causing untold suffering to millions. Kris draws parallels between Long Covid and chronic Lyme and shines a light on how we are being dismissed, misinformed, and deliberately misled by the very institutions that should be protecting us.
 Dana Parish: I’m so excited to welcome Kris Newby. Kris is an award-winning medical science writer and a senior producer of the Lyme documentary Under Our Skin, which premiered at the Tribeca Film Festival and was a 2010 Oscar Semifinalist. Her book Bitten: The Secret History of Lyme Disease and Biological Weapons has won three international book awards. I loved your book so much for journalism and narrative nonfiction. Kris has two engineering degrees and has worked as a science technology writer for Stanford Medical School, Apple Computer, and other Silicon Valley companies. Welcome Kris!
Dana Parish: I’m so excited to welcome Kris Newby. Kris is an award-winning medical science writer and a senior producer of the Lyme documentary Under Our Skin, which premiered at the Tribeca Film Festival and was a 2010 Oscar Semifinalist. Her book Bitten: The Secret History of Lyme Disease and Biological Weapons has won three international book awards. I loved your book so much for journalism and narrative nonfiction. Kris has two engineering degrees and has worked as a science technology writer for Stanford Medical School, Apple Computer, and other Silicon Valley companies. Welcome Kris!
Kris Newby: Thanks Dana, and thanks for having me on the podcast.
Dana Parish: I’m so excited because you are one of the greatest historians of Lyme and you were so helpful to Steve Phillips and me when we wrote our book, Chronic. We loved your book. And Under Our Skin is the film that informed my view of what was really happening with Lyme disease. You’ve been working on Lyme education for 20 years. You’ve done a film, you’ve written a great book, you’ve published articles, you’ve worked in nonprofits, and you recovered from your own tick-borne diseases. How big is the Lyme problem?
Kris Newby: Ginormous and growing. The CDC’s latest estimate is half a million new cases of Lyme disease a year, and I’m sure everyone remembers when Covid hit a half a million. It was like, “Oh no, we have a problem here.” But for some reason, Lyme disease hasn’t bubbled up as a problem. 500,000 cases a year is an average of 1,300 a day. And, obviously, that mostly happened in the summer, so it’s huge. I am often frustrated because I’ve been working in this field for 20 years and not much has gotten better. The disease—this tick-borne disease—if it’s caught early, it can be cured. But we have a test that isn’t reliable in the first month, and later on it’s no better than a coin flip. About 10-30% of the people who are treated with a recommended treatment—according to what study you read—go on to become chronically ill. And the establishment has invested very little in new treatment protocols. I did an analysis with another Bay Area Lyme person of the NIH grants for the last five years, and less than 1% of the Lyme disease NIH budget is spent on treatments.
Dana Parish: That’s shocking.
Kris Newby: I know. So we’re creating an army of chronically ill patients.
“I’ve been working in this field for 20 years and not much has gotten better. Less than 1% of the Lyme disease NIH budget is spent on treatments. We’re creating an army of chronically ill patients.”
— Kris Newby
Dana Parish: I want you to talk a little bit about why that is because I’ve had some pushback when I talk about Long Covid and Long Covid patients, and what’s happening, and how the NIH just wasted over a billion dollars—which was completely predictable—people go, “Well, don’t you want these things to get funded? Don’t you want cures? Don’t you want therapies?” Of course I do! All I’m saying is that the Lyme community has been waiting for 40 years and I don’t know what the holdup is. So, what’s going on?
Kris Newby: Well, I would say it was a tectonic shift in the incentives in medicine that happened in 1980. Willy Burgdorfer, the discoverer of Lyme disease, discovered the causative bacterium in 1980. He published on it in the early 1980s, and what started it is the Bayh-Dole Act passed by Congress into law. The idea behind that was a good idea, but it had unintended consequences. And that is this: “Oh, the federal government taxpayers are investing all this amount in research and when it’s turned into a drug or a test or a vaccine, the government agencies and the universities should share in that booty.” It went wrong because it shifted the incentives for researchers in public health because it formed an unholy alliance between research and pharma. So, for example, with Lyme disease, this was the first new pathogen discovered in quite a while.
AIDS and Lyme disease were actually discovered at the same time. And when the scientists discovered new things about the bacterium and the viruses—like proteins on the surface—then they would rush to patent them. Then they would do patent deals with pharma. In the past, you would share new information about a dangerous pathogen, but now you hid it because you were in partnership with big pharma; it was intellectual property. And we all know how long it takes to get a vaccine, or a test kit, or whatever to market. So, it put the brakes on scientific research, the building up of discoveries, and the combining of minds. So, that happened with Lyme disease. It has been getting worse and reared its ugly head like a weed with Covid.
Dana Parish: A lot of people in the Lyme world know about this Dearborn meeting, but maybe for people who are new to the subject, they could get a little glimpse from you into how it actually happened, how IDSA (Infectious Diseases Society of America) and the CDC and all these different entities became complicit in all of these coverups around Lyme.
Kris Newby: So, the Dearborn meeting was where the testing criteria and the symptom lists were formulated in the interest of fast-tracking a new Lyme vaccine. If you want the gory details of this, the best book to read is called Cure Unknown by Pamela Weintraub. She was there and she interviewed the people involved, but at the Dearborn conference, a vaccine was the number one priority, not cures, which were like a $10 dose of doxycycline at the time. And really with this unholy alliance, the profit motive was a vaccine that you would be forced to take every year. It’s like a big pharma annuity.
Dana Parish: This is taboo all over again with Covid. As you’re saying this, my hair is standing on end.
Kris Newby: Right? Ivermectin, a chief off-patent drug, was just slammed by the vaccine interests. It’s an all or nothing attitude by pharma.
Dana Parish: So, is it that having a safe, generic, early treatment would make the need for the vaccine less pressing? Or would it have derailed the EUA (Emergency Use Authorization)? What does the deal with that?
Kris Newby: I can’t get into their minds because I think of diseases as a person who’s sick comes into the hospital with different needs. If I were the CDC, I would want to prevent people from getting in the hospital with Covid.
Dana Parish: Yes.
Kris Newby: There is no prevention at all. There still isn’t. My husband has Long Covid, and we are just frustrated because there are no solutions for Long Covid people right now. I don’t understand why the medical establishment would do that, but I understand profit motive—whether the people at the CDC or the NIH would admit—was part of it.
Dana Parish: So, what would it surprise people to learn? The list of documents that you FOIA’ed (Freedom of Information Act) that are on your underourskin.com website from your amazing documentary is truly shocking and mind blowing. I remember the first time I read them; I could not believe that this was really happening. Can you talk about that? Who owns these and why should we care?
Kris Newby: Yale owned one of the vaccine patents and the dean or the president of the college says, “We think that’ll be worth $10 million a year to Yale.” That’s significant. $10 million then was a lot more than it’s worth now. So, the patents were owned, and the patents were patents for the vaccine. There were two vaccines. There were also patents for the test kits that supported the vaccine. So, there’s controversy around Dearborn. There were actually two Dearborn meetings where the first time the vaccine wasn’t as effective as they wanted. So, in this Dearborn meeting, they swept the room for bugs and only the people involved in the vaccine trial were allowed in there. And somehow the definition of the disease changed, and the test was desensitized, and you can read Pamela Weintraub’s book for the details. I mean, this is the common understanding and even people who were in that meeting agree.
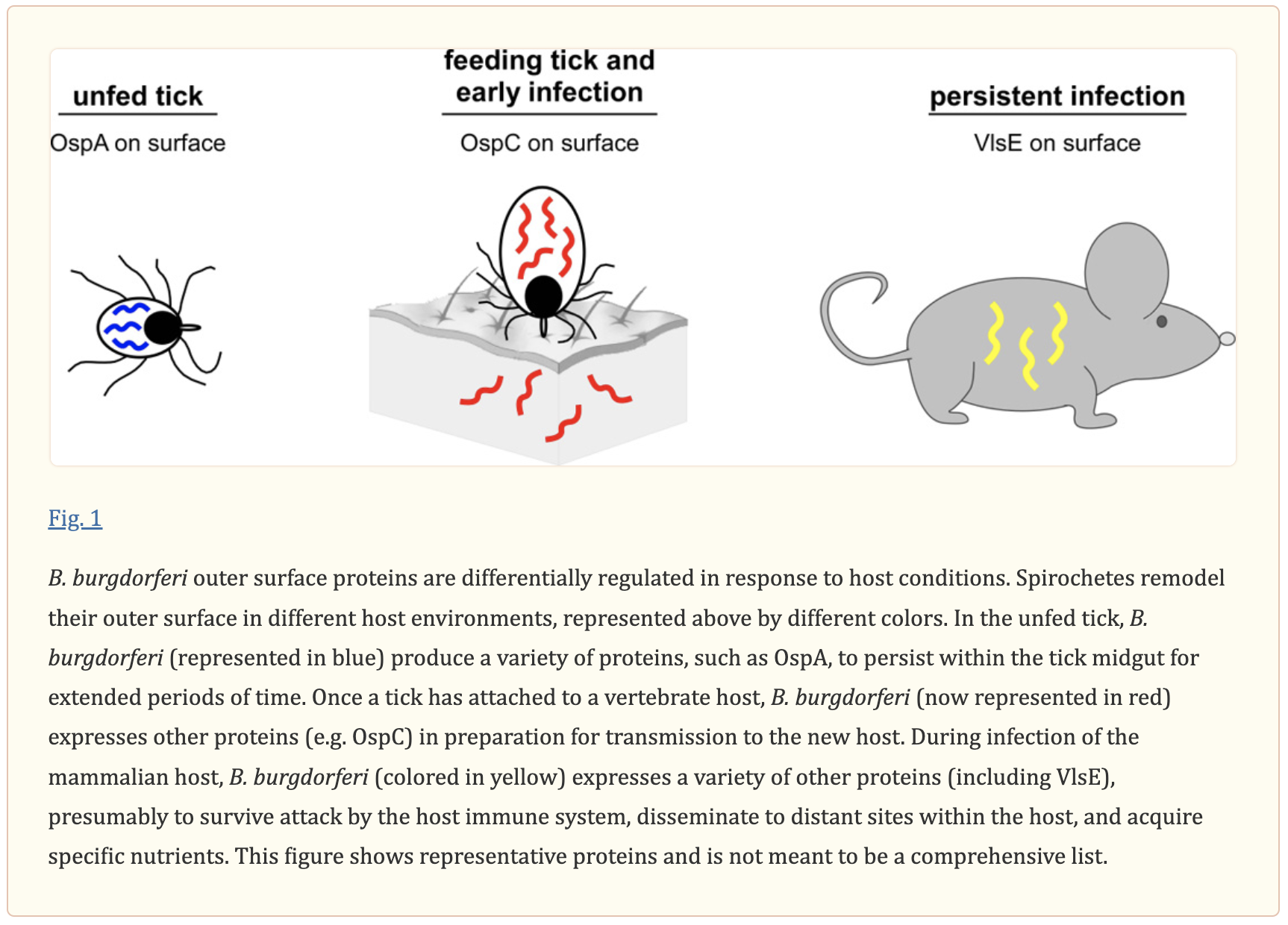
Kris Newby: So, 40 years later we’re stuck with a desensitized test that doesn’t work very well. And this is leading to people becoming chronically ill. And one of the reasons it wasn’t as effective as two of the most specific protein markers on the outside of the Lyme spirochete (bacteria) were used in the vaccines and they were never put back in the tests. So, you’re all of a sudden missing a lot of people who are truly positive, and then people tend to believe tests. They’re accustomed to the AIDS test, which is 95% accurate, and healthcare providers are not used to a test that’s 50% accurate—even frontline physicians who spend 15 minutes on tick-borne diseases in med school. So, there’s an over-reliance on believing tests are real. That’s a problem. And they’ve never put those very specific Lyme proteins back in the tests. So, they’re still missing it.
“We’re stuck with a desensitized test that doesn’t work very well leading to people becoming chronically ill. People tend to believe tests. They’re accustomed to the AIDS test, which is 95% accurate, and healthcare providers are not used to a test that’s 50% accurate. So, there’s an over-reliance on believing tests are real. That’s a problem.”
—Kris Newby
Kris Newby: And even the researcher insiders agree that the tests are really bad, but no one will change it. So, that’s very frustrating to patients. The other thing is the new Lyme vaccine is the same strategy. So, when they were redefining how the vaccine works, in one of these insider meetings, they said, “Well, we thought that the vaccine would create antibodies in a human and then that would fight the Lyme bacterium.” But that wasn’t working because the Lyme disease bacterium is a shapeshifter, it’s pleomorphic, it changes when it senses antibiotics or the immune system. It goes into a dormant cyst form, or it goes into places in your body that your immune system can’t get to, or it hides out inside of white blood cells. It’s very crafty, just like the AIDS virus. And we don’t have an AIDS vaccine. So it’s just the new vaccine that’s in the works uses that same strategy, which I hope it works, but who knows?
Kris Newby: The new strategy was, “Oh, the vaccine takes one-two days to go inside of the tick that attaches, and then like a bellow sucks in blood back and forth and back and forth, and then it kills the spirochetes in the gut of the tick.” Well, the problem with that is sometimes the Lyme bacterium is in the saliva already when it bites you, so you can get it faster than two days before the vaccine works. The other problem I have with the vaccine, which is fundamental, is Lyme disease isn’t the worst tick-borne disease. There are 20 other diseases, like the very deadly Powassan virus that can be transmitted by a tick bite within 15 minutes and there’s not a good test available for that. It gets overlooked. So, that’s just a few of my thoughts. It’s like, “Is the vaccine really solving the problem, which is out-of-control ticks and all the other tick-borne diseases?” There’s some research going on about tick saliva vaccines—which might be better—that would combat all the diseases that are released from the tick.
Dana Parish: Yes, I would agree. I think that that would be a really worthy endeavor. Even Durland Fish was quoted in Yale magazine saying that another Lyme vaccine really doesn’t make sense because of all the reasons that you state. Also, there are a lot of different strains of Lyme, and I don’t know that they’re all going to be even covered with a new vaccine. There are a lot of problems, and there’s just so much misinformation/disinformation in the whole world of Lyme. It’s the craziest thing to watch if you’re new to it, if you’re sick with it, and you learn about it; it’s sort of mind blowing. Why is there so much literature that demonstrates that Lyme is chronic, that Lyme can become chronic, it can hide in organs, hides in tissue just like Covid, just like many, many other pathogens, and then all of a sudden there was this shift and it was denied? What is the motivation to deny the perniciousness of Lyme?
Kris Newby: Well, you have the force of Pfizer and Valevna behind this new vaccine, and it’s built on the bad foundation of research, the bad tests, and the falsity that Lyme disease can’t be chronic.
Dana Parish: Why does it matter that Lyme is chronic when it comes to the vaccine? That’s something people ask me to clarify all the time. I’d like to hear it from you.
Kris Newby: If you want to run a scientifically valid vaccine trial—and I worked in the clinical trials group at Stanford for 10 years—you have to have a reasonably accurate test, and you can’t necessarily have a disease that can go dormant in your body for months to years. That’s what the new primate research out of Tulane by Monica Embers is showing. She gave the equivalent dose of doxycycline to primates, our closest living relatives, and a year later the Lyme disease came back and in some cases the monkeys who were treated with doxycycline had worse neurological involvement from the Lyme disease. So, the antibiotics just chase the germs into the brain and make the situation worse. So, why are they ignoring it? Well, a lot of these people that are saying Lyme disease is easy to diagnose, treat and cure, have their fingers in the vaccine till. I’ve been in this for 20 years. Pam Weintraub has been in it longer. There’s this group bias that’s happened and an “us-versus-them” political divide that is as bad as the Republicans and Democrats. For example, I dug up some quotes from the people who are in that academic research world, and I’ll just read some of them.
“A lot of these people that are saying Lyme disease is easy to diagnose, treat, and cure, have their fingers in the vaccine till.”
—Kris Newby
Dana Parish: Please do.
Kris Newby: One of them said, “Lyme disease is primarily a disorder of suburban, educated, middle- and upper-class people.” And he said this in the Journal of American Medical Association
Dana Parish: Who said that?
Kris Newby: That was Alan Barbour.
Dana Parish: Oh my God.
Kris Newby: Then Steven Ostroff, who was in CDC, said to a group of Illinois legislators in 1997, “Lyme disease is a yuppie disease which only rich suburbanites get.” Then there’s Eugene Shapiro at Yale who believes that if parents insist that their kids have Lyme, the parents could have Munchausen by Proxy where you make your kids sick to get attention, it is usually not Lyme disease unless it looks, smells, and tastes like Lyme disease. There’s Lenny Sigel from the Robert Woods Johnson Foundation who is highly funded. He said in the New York Times in 2001, “Lyme disease, although a problem, is not nearly as big of a problem as most people think. The bigger epidemic is Lyme anxiety.” And so, it goes on and on. I have 17 pages of these.
Dana Parish: It’s the same thing with Long Covid now. I’m already seeing that kind of language.
Kris Newby: It’s true. It creates a mindset all the way down the medical healthcare provider ecosystem that makes people not believe the patients.
Dana Parish: That’s true.
Kris Newby: It’s been really destructive and it’s the “us-versus-them” thing, so they’re just not listening to the patients. And finally, we have the scientific evidence from Monica Embers’s work at Tulane, for example, that is making them look. But underfunding is a huge problem because the funding in Lyme disease—and I really drilled down deeply into this in the documentary—is primarily going to basic researchers. So just understanding tiny molecular mechanisms and not cures.
Dana Parish: Yes.
Kris Newby: 60% is basic research and the grant review process from the NIH is totally broken and the insiders know that. You have these researchers who are MD/PhDs, they’re the smartest people in the world, and they figured out how to game the system. When I was doing the research with the film, I realized that it’s like figuring out the family ties in the Mafia. Because there’s no org chart that says, “Oh, this guy’s a good fellow who’s a friend with this good fellow.” So, I just got all the publications and who gave grants from one university to a buddy at another university, and there was obvious collusion, and that really was part of the basis of the Attorney General’s suit against the Infectious Diseases Society of America with the Lyme cabal.
Dana Parish: This is organized crime as far as I’m concerned. I’ve always looked at it that way, and now I’m seeing it again playing out with Covid.
Kris Newby: Well, the IDSA suit in Connecticut was a RICO suit, and this week everybody knows what RICO is. It’s racketeering.
Dana Parish: I want to talk to you about that. I want to talk to you about a case that’s going on right now, a little bit later today. So, here’s one thing that I have said many, many times, and I think it would be great to get a little more context from you. The IDSA guidelines are bad. I got chronically ill—I’m actually okay now—but I got very, very sick and went into heart failure because the doctor that I saw at the urgent care followed the IDSA guidelines and gave me three weeks of doxycycline, and didn’t look for any other vector-borne diseases. I had a second one that was missed for five months, and she told me not to Google Lyme disease because she didn’t want me to become a crazy Lyme person. I didn’t even know what that was. Can you talk about why the IDSA guidelines are so wrong?
Kris Newby: I think the IDSA was formed just after Lyme was discovered, but the Infectious Diseases Society of America, they are largely funded by pharma who buy expensive booths at their conferences, expensive ads in their journals. And pharma has seen these medical societies as a way to promote new drugs and guidelines, which are one-size-fits-all, are the perfect way to push their new drugs.
And also IDSA serves as sort of match.com for vaccine and drug trials and the people that would manage those—which are academics in high prestige medical universities. Again, an unholy alliance, the people who are infectious disease people are specialists and they don’t take care of run-of-the-mill patients. They’re like bubble boy people. They come in, someone’s dying, they give them their very powerful antibiotics. By the way, they’re running out of very powerful antibiotics because of resistance and how dare those Lyme patients want to be on antibiotics for months to year because it brings them so much joy taking antibiotics.
Dana Parish: And of course, they’ve come up with nothing else. And of course, the most egregious use of antibiotics is agriculture. So, 80% of antibiotics go into our land, into our food, it’s sprayed all over our crops. Nobody talks about that. They talk about Lyme patients. Isn’t most of the resistance also coming from hospitalized patients with MRSA and other resistant diseases?
Kris Newby: The infectious disease people mostly work in those sort of ICU situations in those institutions. And what happened recently is Medicare/Medicaid refuses to reimburse medical institutions where the MRSA or whatever originated in the hospital. That’s another reason not to want to use a lot of antibiotics on the outside, even though that’s misinformation. It’s agriculture. We are giving antibiotics to fish that we grow for food. And the amount going into agriculture is increasing in the next one or two years, according to this latest study I read.
Dana Parish: It’s so disgusting what they’re doing and how polluted and toxic all of this world is and all the money being made to basically poison us. One thing that I learned from you was about astroturfing, and I think we should talk about that because there’s so much propaganda. I think it’s really hard for even the most critically minded, well-intentioned people to separate fact from fiction because the Lyme wars are so challenging to discern. What’s the deal with astroturfing? Who’s doing it and what can we do to combat this incredible amount of misinformation that they’re putting into the world?
Kris Newby: It’s a bad problem. “Astroturfing” is getting worse with AI, but I’ll just use the American Lyme Disease Foundation (ADLF) as an example of this deceptive practice.
Dana Parish: The worst of the worst.
Kris Newby: They put up a website that says, “We care about Lyme disease; we care about patients.” But it’s really a website to post their point of view about the disease and mislead journalists—in my opinion. When I was doing research for the documentary, I drilled down, searched the internet protocol to find out who’s paying for that website. At that time, the website was being run at an office on the Yale campus. So again, remember it is Yale who has a financial finger in the pie, the royalties from the test kits and running vaccine trials, and the office was also being staffed by people from New York Medical College who have a certain view about Lyme disease, which is: “Lyme is easy to treat and cure. If people have chronic Lyme, it’s because they’re suffering from past life trauma.”
Dana Parish: Who started this? Who were the players that started this campaign?
Kris Newby: Well, the people who are still on the board are Gary Wormser and Alan Barbour. It’s still based out of Yale. I think now it’s a front for information promoting the vaccine and it’s well funded by Pfizer. The woman who was just named director is called Andrea Love. She runs this science podcast called “Unbiased Science” that goes on and on about things like, “Oh, it’s okay to eat GMO food.”
Dana Parish: And Teflon is good for you.
Kris Newby: And chronic Lyme doesn’t exist. And these people are being duped by buffoons and quacks.
Dana Parish: She’s very dangerous. She’s very, very dangerous. I am reading some social media posts that she put out. She’s a microbiologist. She was under the tutelage—as far as I know—of Gary Wormser.
Kris Newby: He was a reviewer of her thesis.
Dana Parish: There you go.
Kris Newby: Her newly minted thesis.
Dana Parish: Totally. Her thesis is about how Lyme evades the immune system. It’s about how Lyme becomes chronic. Here’s the question that was posed to her, or that she posed to herself. “If Lyme disease went untreated, could it present years later? If so, how?” Here’s her answer: “No, this wouldn’t happen. Most infections will self-resolve even without antibiotic treatment, but untreated infections would not suddenly reappear. There is a common fallacy among the chronic Lyme community that these bacteria become dormant in the body, but that is not true.” That’s nuts. That’s just a complete lie. How do people like her get away with this? One thing that should be noted is that there is a disclaimer on her website—on their website—saying that they can’t be held accountable for anything they say. They’re not MDs, they’re not advising on treatment. They’re advising not to treat a tick bite? They’re advising not to treat an initial infection that can cause you to become completely disabled, or even die? How are people getting away with this and just no consequence?
Kris Newby: I don’t know. We need to call them out on social media, so they’re informed. They have a powerful Wiki presence and we need to shine a light on what they’re doing, I think. But here’s an important thing for patients new to Lyme disease to know, and that is there are different kinds of MDs. Not all MDSs are created equal.
Kris Newby: If you’re new to Lyme, you’ll go to your primary care provider who isn’t set up to take care of a chronically ill patient. They will boot you to a specialist. The specialists aren’t incentivized to take care of a chronic Lyme patient who has multiple organ systems, and the treatment at first can be worse than the disease and must be monitored so the patients don’t die of sepsis from killing off all those germs at once. And the whole insurance structure is not designed to deal with this kind of patient. The one exception is cancer centers that deal with this. They have social workers, they have nurses to monitor the drug reactions and adverse effects, and that’s what needs to happen with Lyme disease. We need the cancer center model. But the thing about cancer drugs is you might have to mortgage your house to pay for those treatments.
“The whole insurance structure is not designed to deal with this kind of patient. The one exception is cancer centers. They have social workers, they have nurses to monitor the drug reactions and adverse effects, and that’s what needs to happen with Lyme disease. We need the cancer center model.”
—Kris Newby
Kris Newby: There’s a profit incentive with Lyme disease. Why? Because it’s a very cheap cocktail of several antibiotics to kill the spirochete form. So, there are two kinds of doctors: 1)The McDonald’s order-taker pushing you up to the specialist. You end up going to 10 different specialists. None of them know what to do with you because the medical journals and a lot of the textbooks are wrong. They haven’t kept up with the new science. And that’s why people end up going to the other kind of doctor: 2) the Lyme specialist because the Lyme specialist has seen five or 10 thousand of these patients and they know what has to happen and that it’s going to be a long process. The Lyme specialists do not take insurance a lot of times, mostly, because they know they will reject them and the patient will get sicker and sicker with brain inflammation, maybe Lyme carditis, and those Lyme specialists say, “We don’t take insurance because it kills our patients.”
Dana Parish: Well, that’s true. The irony is that when you listen to people and things like the Unbiased Science podcast, or the ALDF people, they gaslight their audience into believing that: “These people are predatory and they’re trying to make money.” Well, who funds them? Go and look up all of the physicians that you may know that are working in mainstream hospitals. And by the way, I did this when we were writing our book. I found out that a rheumatologist that I saw from Hospital for Special Surgery in New York made like $700,000 from biologics just from basically doing talks. And when I say biologics, I mean Enbrel and drugs like that. These are things that a lot of Lyme patients get relegated to because their infections are not treated early and they go on to have rheumatic diseases, neurologic diseases, psychiatric diseases. So, I always say chronic illness is a cash cow.
Dana Parish: If you don’t treat Lyme patients, many of them are going to go on to have autoimmune, psych, neurologic diseases, and cardiac diseases. Perhaps in the face of Covid, there is a new awareness of what a multisystemic, common, wily, immune-invasive infection can do. But prior to this, you would just get crickets. I would try to educate a new doctor about what happened to me and talk about what happened to my brain, what happened to my heart, how my hands and feet were tingling and how I could have been diagnosed with MS or Parkinson’s. I had a tremor and all kinds of neuropsych stuff and visual disturbances, and yet a few months of antibiotic treatments shut it all down. I don’t take any medications anymore. But had I not kept seeking answers, and had I not been fortunate enough to see a tick bite and a rash on my shoulder, I would be for sure, probably a pretty seriously ill chronic illness patient—even if I had lived because of my heart failure. People don’t understand that this is actually the truth of what’s happening, and I think these conversations are so important.
Kris Newby: The advice I give a lot to new Lyme people is: Don’t try to change the mind of an infectious disease doctor.
Dana Parish: Absolutely.
 Kris Newby: You don’t have the time. In the world of strokes, you say, “Time is brain.” You’re going to lose your brain if you don’t act quickly. And so, it’s going to cost you upfront, but not over the long term if you wait and try to work in the system as broken as it is now. This is with Long Lyme and Long Covid, and so my husband and I ended up at a lot of these new institutions. They put up a shingle or just a pseudo website that says they have a “Long Covid clinic.” In my area at the Long Covid Clinic what they offered was talk therapy—no drugs, no solutions. We read the FLCCC site on Long Covid, and there were some ideas there, and they have worked. I mean, my husband didn’t have taste or smell for two years. Two or three things helped, and I don’t think there are many clinics that are doing it, but he went to the low-pressure hyperbaric chamber, which helped healing. He had NAC (N-acetylcysteine) drips at just one of those commercial labs staffed by nurses, and that helped. And then for his ADD caused by Long Covid, Gabapentin has helped flatten the nervous system a little.
Kris Newby: You don’t have the time. In the world of strokes, you say, “Time is brain.” You’re going to lose your brain if you don’t act quickly. And so, it’s going to cost you upfront, but not over the long term if you wait and try to work in the system as broken as it is now. This is with Long Lyme and Long Covid, and so my husband and I ended up at a lot of these new institutions. They put up a shingle or just a pseudo website that says they have a “Long Covid clinic.” In my area at the Long Covid Clinic what they offered was talk therapy—no drugs, no solutions. We read the FLCCC site on Long Covid, and there were some ideas there, and they have worked. I mean, my husband didn’t have taste or smell for two years. Two or three things helped, and I don’t think there are many clinics that are doing it, but he went to the low-pressure hyperbaric chamber, which helped healing. He had NAC (N-acetylcysteine) drips at just one of those commercial labs staffed by nurses, and that helped. And then for his ADD caused by Long Covid, Gabapentin has helped flatten the nervous system a little.
Dana Parish: Oh, that’s great. Those are great tips because a lot of people that are going to watch or listen to this are going to be needing some insight into how some people have gotten better from those symptoms. It’s horrible. I mean, do you think about a billion dollars went to funding Long Covid? And what do we have to show for it?
Kris Newby: Well, that’s the latest scandal with Covid. Nothing. That money goes to universities that cream off 45-65% of the research dollars for university infrastructure. The thing that’s been pointed out recently with Alzheimer’s is a lot of that money goes to basic research and funding the predominant theory of: What’s wrong? For example, regarding that one billion dollars, one of the studies was asking the question, “Does exercise hurt or harm Long Covid patients?” And if they had just talked to the patients, they would have said, “We can’t exercise! Why are you studying this?” So, I don’t know how these decisions are made, but things would be better if you listened to the patients. These patients are not lazy. They want to get back to work more than anything.
Dana Parish: Who would make this up? Who would fake this? So many of us are at the prime of our lives when we get completely derailed, and it is like déjà vu watching this whole thing unfold with Long Covid. It’s horrifying. And then what I find also really upsetting is that so many people don’t believe Long Covid is real. Just like they don’t believe chronic Lyme is real. I don’t understand that at all. Do you not believe breast cancer is real? Do you not believe in HIV? Some people, yeah, they don’t believe HIV is real either. I have never seen anything so crazy in my entire life as this denial of the experience of millions and millions and millions of people and counting. And speaking of epic fails, I want to talk about the CDC response to the Covid pandemic and how it relates to what we’ve been through. Why are we not surprised? Why are we not surprised as Lyme patients?
 Kris Newby: Well, as part of the research for my book Bitten, I went deep into the CDC history and something people don’t really realize is the CDC was originally founded after World War II as a sentry to be on the lookout for biowarfare attacks from bad actors like the Soviet Union. So, secrecy is in its DNA. Then over time because they want more money from Congress, they’ve expanded their scope of influence, and they’ve gotten away from the core purpose, which I think would be important, which is controlling epidemics. And they are a bloated bureaucracy right now. Now, I know some people in CDC. I love them dearly. They have the patient interest at heart, but they’re trapped inside this bureaucracy. And the CDC has fallen behind in technology. Their surveillance was pathetic with Lyme disease. It seemed like they had designed an overly Byzantine reporting structure for Lyme disease. It was designed to lose cases. And only when they looked at the insurance records did they go, “Uh oh. we’re way off-base.” And it seemed like the local health departments and state health departments thought they would make CDC happy by under-reporting and throwing stuff in the waste bin. But anyways, they weren’t doing good tracking. The veterinarian side of the government is doing better tracking for Lyme disease because there’s no bias in that.
Kris Newby: Well, as part of the research for my book Bitten, I went deep into the CDC history and something people don’t really realize is the CDC was originally founded after World War II as a sentry to be on the lookout for biowarfare attacks from bad actors like the Soviet Union. So, secrecy is in its DNA. Then over time because they want more money from Congress, they’ve expanded their scope of influence, and they’ve gotten away from the core purpose, which I think would be important, which is controlling epidemics. And they are a bloated bureaucracy right now. Now, I know some people in CDC. I love them dearly. They have the patient interest at heart, but they’re trapped inside this bureaucracy. And the CDC has fallen behind in technology. Their surveillance was pathetic with Lyme disease. It seemed like they had designed an overly Byzantine reporting structure for Lyme disease. It was designed to lose cases. And only when they looked at the insurance records did they go, “Uh oh. we’re way off-base.” And it seemed like the local health departments and state health departments thought they would make CDC happy by under-reporting and throwing stuff in the waste bin. But anyways, they weren’t doing good tracking. The veterinarian side of the government is doing better tracking for Lyme disease because there’s no bias in that.
“The CDC has fallen behind in technology. Their surveillance was pathetic with Lyme disease. The veterinarian side of the government is doing better tracking for Lyme disease.”
—Kris Newby
Dana Parish: Oh, absolutely.
Kris Newby: And then there are the communications. All Lyme patients knew this was broken on the CDC end. Then Covid came along and there were more body bags, so they noticed, and they couldn’t write off the patients and say, “Oh, this patient was just faking death.” They just completely crumbled with communications too. This is our very dysfunctional political system. If they had just done what Andrew Cuomo had done in the pandemic, which is: just get on TV once a week or twice a week and explain the numbers. It’s like none of the people at CDC did math or anything that gives us the numbers or gives us the straight story. It’s such a horrible thing. And then the other thing we found is this group bias. I mean, I read some things from the CDC earlier, the quotes. They believe that all Lyme patients are faking it. And now Long Covid probably, and there’s a revolving door between pharma and CDC. The CDC salaries aren’t that great, but you go to pharma and it’s just like 10 x your other salary. And of course, pharma would want to engender that because then they have more chance that their drugs will be accepted and promoted by the CDC and the NIH.
Dana Parish: It is so corrupt. It’s so huge. I mean, it is really a problem that just feels insurmountable. I know you called me the other day, you said: “Don’t give up! We have got to keep chipping away!” And I think you’re right too. I think both things are true. We have to keep telling the truth. But we are up against big, dark, extremely well-funded forces. You do feel this weary familiarity watching this happen with Long Covid. And that leads me to want to talk to you about your book Bitten, and biowarfare, and gain of function research. What is it? What have we gotten out of it? And how does the bioweapons angle of your book relate to Lyme?
Kris Newby: The thing I discovered that launched the book was that Willy Burgdorfer, the man who discovered Lyme disease, was brought over from Europe specifically for the bioweapons program after World War II.
Dana Parish: Where was he from?
Kris Newby: He was from Switzerland. He was Swiss German. His dad was a Nazi hunter. He came over and he had worked on ticks and Q Fever in Europe. Q Fever was the go-to bioweapon then. He went to Rocky Mountain Labs in Montana and his job was to weaponize fleas, ticks, and mosquitoes. That involved injecting ticks with various horrible diseases, rabies, Venezuelan equine encephalitis, relapsing fever, and Tularemia. He would be given objectives through his boss for (Ft.) Detrick objectives: “Okay, we want a tick that can survive Siberian winters and won’t attract a lot of attention because it looks like a native tick.”
Dana Parish: Let’s clarify why you would do this.
Kris Newby: Well, after the surrender of the Japanese and the Germans, they realized that the Japanese were developing all sorts of insect-borne weapons and the Germans were doing some too. And it made them paranoid because the Soviets had stolen some of those scientists too, and it’s the perfect stealth weapon. Let’s say you’re planning on invading Russia, you would drop these infected ticks, or fleas, or mosquitoes, and it would weaken the local population, tie up medical resources. There’d be no fingerprints on the ticks, so you wouldn’t know who had done it even if it was diabolical.
Dana Parish: Right.
Kris Newby: And then you could go in with ground forces and take over the infrastructure. No buildings would be destroyed by the ticks or fleas and mosquitoes, and you could get the locals’ expertise to run the power plants or whatever. That was the objective. There are many documents supporting that. And then with the research, Willy Burgdorfer donated some of his original bioweapons’ documents to an archive at Utah Valley University. All his archives are online now. I got to those before they were posted because it takes a long time to post them. So, I got to see his original lab notebooks and letters talking about these programs.
Dana Parish: What was most surprising that you learned from reading those?
Kris Newby: That they were weaponizing, Rocky Mountain Spotted Fever, which is the most deadly tick-borne disease in North America.
Dana Parish: When you say they were weaponizing it, were they conducting experiments that could make it more dangerous and possibly more contagious, or that other insects could carry it? Or were they taking the natural infection and releasing it? What were they doing?
Kris Newby: It goes back to what you’re saying about gain of function, and they said, “Willy is working on these.” Well, in mosquitoes, for example, he was working on a really deadly Trinidad agent virus that had been brought over from Trinidad, and he was putting it in animals and trying to find the most virulent or lethal dose. That is an example of very crude gain of function.
Dana Parish: What could go wrong?
Kris Newby: I know. And then later on, the gain of function became more sophisticated. In the mid-sixties, the University of Wisconsin was doing it at a genetic level, mixing viruses and bacteria. Willy did mix bacteria and viruses inside of ticks. So, that is what I would call gain of function. Fauci slices it more narrowly, but they say: “We are breeding these germs to make them more virulent.” Now, one of the main finds of the book is that Willy Burgdorfer, when he was investigating the Lyme outbreak in the mid-1970s, said that he saw a rickettsia that he thought might have been a bioweapon that his lab worked on earlier. Rickettsia is a very small intracellular bacteria, part of the Rocky Mountain Spotted Fever family. He was told to hide that in his science article announcing this discovery. Then all of a sudden—in the middle of the investigation—he flew to Switzerland. He collected 4,000 ticks, and found this thing called the ‘Swiss Agent’ which was a rickettsia, developed a test based on that, and he said almost all of the Lyme bloods that he was given to analyze were positive for this Swiss agent.
Dana Parish: Wow. And that was all over the world? Or just US-centric? Or?
Kris Newby: Well, the ‘Swiss Agent’ was in Europe. The question is, where did it come from? Was it a Nazi rickettsia that got out? Was it something that we dropped on over the Iron Curtain or…. we don’t know. But it reacted to the test. The US version reacted to the test. And the thing that Willy thought…. I mean, when you publish an important scientific paper, you say, “I think it’s the spirochete, but we found these other organisms in the ticks and the humans.” He should have said that. It got pulled (redacted). I saw his handwritten draft of the article before it was published, and he said there was this mysterious rickettsia. There was a nematode worm, and somehow the ‘Swiss Agent USA’ disappeared and has never been mentioned again. Now, Willy claimed credit for the discovery of the ‘Swiss Agent’ in Europe and got credit for that, but not the US version.
Kris Newby: And so why was that organism buried and was it contributing to why people were getting sick in that area? So, the other thing that was outrageous to me in the research of the book was that Lone Star ticks before the mid-1960s were mostly just in the South, below the Mason-Dixon line. They hired the Army and the Atomic Energy Commission hired a young and overly ambitious researcher at Old Dominion University to release hundreds of thousands of ticks that are made radioactive, including the Lone Star ticks on the Atlantic Bird Flyway. He released them. And every month he would go back and use a Geiger counter to figure out how far they’d crept, or crawled, or flown on birds. And then he would put them back in the squares, the bigger ones he would paint. So, a year after that, all of a sudden Lone Stars became established in Long Island in the north, and there was a horrible spotted fever epidemic. People died, people got really sick, and is there cause and effect? Why aren’t epidemiologists and tick researchers looking into this? Because they’re funded by the NIH.
Dana Parish: I was going to say, this is just such a scandal. People don’t know about this. What are your thoughts? When I got Lyme, I was waiting in a doctor’s office to be seen, and there was a woman in a wheelchair sitting next to me who had MS, and she said: “I got MS from untreated Lyme. Do you know that Lyme was leaked from Plum Island? And that’s how it got to Lyme, Connecticut, and to Montauk right across the water?” And I had never heard about it, again. I was new to Lyme. I was extremely ill, but I was horrified by what I heard. What’s the deal with Plum Island and is there truth to that?
Kris Newby: Well, I have some of the oldest case records of the outbreak of Lyme disease, and definitely the point source outbreak was the mouth of the Connecticut River and Thames River, and you can see Plum Island from the old Lyme Beach Club.
Dana Parish: What was happening there? I should have given a little background.
Kris Newby: Plum Island is now owned by the USDA. It was the headquarters for anti-animal bioweapons—that means our strategies for killing livestock to starve an enemy population. They did have a tick hatchery there. Plum Island did have a lot of safety breaches. They weren’t that careful, and they weren’t working on spirochetes, as far as I can tell. They could have been working on something close to Babesia, which just showed up at the same time as Lyme disease along with the Rocky Mountain Spotted Fever in the late sixties.
Dana Parish: Just to be clear: three new diseases unknown to us showed up at the same time in the same place within a certain proximity to Plum Island.
Kris Newby: Yes, in the late 1960s, which was the height of the bioweapons program. It was shut down by President Nixon in 1969, and then the stockpiles were destroyed in 1972. Now, it could have come from Plum Island? I could not find any proof—except for proximity—for those three diseases. So, we’d need some disclosure there if the records haven’t been incinerated.
Dana Parish: It’s pretty curious, I would say. What was the pushback like for your book? I can only imagine when you published Bitten that you had a lot of people on edge that didn’t want this information to be put into the public domain in such a big way.
Kris Newby: I would say the research was hard. My realization of the size of the disinformation machine was jaw dropping. I couldn’t believe it. So, it didn’t get a lot of advanced reviews. It was a very touchy subject, and I didn’t want to leak out what it was about sooner than it had to be. And then it just sort of rolled out. It was popular amongst the Lyme community, but a few weeks after it came out, Republican congressman Chris Smith of New Jersey was in the middle of the Department of Defense budget negotiations, and he held the book up on C-span, which is an international TV channel. Everyone who’s interested in getting into the military industrial piggy bank watches that. And he said: “This is a really credible book. The allegations of weaponizing the ticks are important because really we can treat it better if we know what was released where, and when.” You don’t have to have people dragging with bed sheets all over the United States. You can just hear, “Okay. They released something that looked like anaplasmosis in Wisconsin. Let’s study that.”
So, that created a firestorm. I was still working as a science writer at Stanford. It was chaos. And then the disinformation campaign kicked in. Soon after this, a tick researcher from Tufts, Sam Telford published about a thousand word op-ed that ran in the Washington Post unchecked that said pretty much everything in my book was conspiracy theory. We never released any weaponized anything in the United States or anywhere else, and on and on. So, I called him right after I said, “Sam, did you read my book?” He responded, “No, I don’t have time to read books.” But he teaches biosecurity at Tufts, and he’s a tick expert and some of his lies, I mean, I analyzed it in detail and it’s on my website, Krisnewby.com rebutting what he said in this op-ed. There were 15 outright lies or mistruths and this guy should know. And so, I said, “I’ll send you a book.” And he says, “Oh, no, don’t send it to me. I will just shred it.”
Dana Parish: Shred it literally?
Kris Newby: I don’t know. I did not waste a book on him after he said that. So, not an open-minded guy, or maybe he knows, and he’s paid. The other thing he didn’t disclose in this op-ed is that research threat, tick-borne weapons, select agents that are a threat to the United States, including Tularemia. He didn’t disclose that. So, then I called the science editor at the Washington Post. I said, “Did you know this guy wasn’t telling the truth? He’s a professor, a tenured professor at Tufts!” And the science editor said, “Well, we just republished from this other news site for free, and we don’t fact check op-eds.” Even though their Washington Post stated policy says: “We fact check op-eds and we require that our authors disclose conflicts.” So, I don’t know, this is just what’s going on with Covid. There are other journalists who’ve been treated worse. But this op-ed effectively killed a movie deal for the book and killed book sales. And all of a sudden on the internet, this misinformation from the conflicted biosecurity professor and director proliferated across the internet, and I can’t scrub it. I’ve been back to the Washington Post three times. The ombudsman, the editors, won’t correct it or remove it.
Dana Parish: Part of the disinformation warfare information warfare that has happened with Covid, that happens around bioengineered pathogens and that happens around biosecurity, it’s very creepy. I’m not surprised that you can’t get it removed. And I’m not surprised that there would likely be government fingerprints all over that. Of course, Sam Telford knows. Of course, he knows that what you said in your book is true. I mean, you have so much evidence, you have so many historical documents, and it’s ludicrous if you read the book, it’s like gaslighting 101 to say that it’s not credible. It’s just breathtaking what they get away with. What do you think about the origins of Covid?
Kris Newby: I haven’t studied it, but when I heard about it based on my five years of research, it’s like, of course it could have been a weaponized thing. It seems like more and more evidence is pointing to that it was initially funded by the US, but it was moved to Wuhan. Wuhan had many safety issues, but I don’t know if we’ll ever know the truth.
Dana Parish: Again, here we are with an incurable chronic infection. It’s disabling so many people and no answers. Maybe if we knew where it came from, we would’ve a better sense of how to treat and cure it. And there’s the issue of it reactivating other latent infections and it’s such a mess.
Kris Newby: Every day I think about how can we fix the situation, both the Lyme and the Long Covid situation, and it is hard for one person to do it, but I think funding independent journalists that will tell the truth like ProPublica is really important because the institutional corruption is just like roots of weeds, deeply buried, and we cut off this head and this head, but it’s still there and we need more. I am on all the investigative reporter feeds, and more and more investigative reporters are getting laid off. How are they going to get paid? This is such an important function for healthy democracy.
Dana Parish: There’s so much corporate influence. I was talking to a couple of mainstream journalists recently who said they know what’s really happening with Covid. They have strong opinions about Covid origins. They have strong opinions about what happened around vaccine misinformation saying that the vaccine was going to stop the pandemic and stop transmission. They also know about lying, some of them, and they say they can’t report on it because they have to get it through their editors. It’s just such a long line of people. And there are intelligence people involved. One thing that is also not known, is that there are intelligence people planted all throughout the media. So, they can shape a story, kill a story—hashtag Sam Telford—and they really do change the public’s perception of what’s happening in the world now and historically. So, before we go, I want to talk to you a little bit about the Lyme lawsuit, but also just about what’s happening in the media at a high level and who is there controlling the narrative?
Kris Newby: Just turn on CNN and count the drug ads. And there’s been a recent article—now, I haven’t fact checked this—but Anderson Cooper is funded $18 million a year, and $10 million of that is from Pfizer. But I haven’t fact checked it.
Dana Parish: I read that headline. Is that true? I didn’t look into it. I don’t know.
Kris Newby: I don’t know. But just look at the drug ads. So that’s got to play into what they cover and what they don’t cover, and it’s not easily traceable. Then the few reporters and major media that exist, that are national security, the government, etc., rely on sources to feed the monkey—to publish new stuff every week. So, if someone in the inside government says, “Steer away from that Lyme story,” they’ll do it because they need that source to have an open conduit. So that’s part of it.
Dana Parish: And I think sources misinform as well.
Kris Newby: Yes. Again, my new book goes into the mechanism of coverups from right after World War II, and I have a document that’s from the CIA, that says, “Oh yeah, we have 400 plants in major media. We have this stuff covered.” The way they decide what to cover is that they have an editor’s table, and someone says, “Oh, I want to cover this military accident.” And then their plant would say, “I wouldn’t do that.” The influence is subtle. And for example, the conversation—which is on the surface of nonprofit—is in actuality a pay-to-play publication. So, universities and people with agendas pay them and they may or may not report it on their website… I couldn’t find all the funders. And then they give away free news, and then people like the Washington Post, just pass it through without fact checking it.
Dana Parish: Diabolical.
Kris Newby: I know.
Dana Parish: It’s unbelievable. Here we are doing this podcast, and I hope a million people hear this because they need to know. They need to know how the propaganda machine works. There’s a great article if people want to Google it, called the Propaganda Multiplier by a European nonprofit. The references and the information in this article are phenomenal, and they give you great insight into how stories get syndicated. Misinformation gets syndicated all over the world, and it becomes the truth as people know it. And we see this over and over again. So, before we go, I want to talk to you about this federal lawsuit filed by a group of Lyme patients. What is the status, and what’s going on there?
Kris Newby: This is a lawsuit where this chronic Lyme patient, Lisa Torrey, is the head of it. It’s Torrey versus IDSA, and it’s 21 chronic Lyme patients against the IDSA institutions in the insurance company. It essentially charged that six Lyme researchers have been in cahoots with the insurance companies to deny appropriate medical treatment to patients with Lyme disease in that these Lyme people would be consultants to insurance companies and deny claims for chronic Lyme. So, the institutions like Kaiser all settled, but the IDSA has lots of lawyers and they’re just holding on for dear life. The latest thing was denied on grounds of not enough evidence, and then this fall, the evidence will be presented in a federal court to a judge for the appeal. So, we’ll know this fall if the suit is going to go forward. And why is this important? Because it’s been so hard for Lyme patients to get disability insurance or coverage at these institutions because there’s no precedent. So, this would be a very powerful precedent to help these patients get treated.
Dana Parish: It’s great that they did this, and I hope to see a lot of success around this case. It would be an important precedent to set.
Kris Newby: There was another case about a 17-year-old boy who had obvious signs of Lyme carditis. He was at a camp. He died—I think partially because of his race. He was dismissed. And that went to trial, but they settled. That’s a little bit unfortunate because the depositions from the people involved are not released to the public.
Dana Parish: I remember that case. That was horrific.
Kris Newby: His future was bright and just cut off because, “Oh, that kid’s on drugs; he’s faking it.” Who knows?
Dana Parish: It’s mystifying. It’s such a crime. I’m really worried about gain of function. I’m really worried about Covid and all the experiments now going on with Covid and worse diseases with a higher death rate, and all these ominous warnings from people saying, “There are worse pandemics coming.” Is there anything we can do to stop this? Like this organization BiosafetyNow, where the goal is to put some parameters around this research. Is it transparency? What do we need to do to try to get this to stop?
Kris Newby: Well, this is the pep talk I give myself every day. I’m just one person. What can I do? And I’ve been reading an excellent graphic novel called On Tyranny by Timothy Snyder, who’s written many books on fighting tyranny in government, and everybody has to do their part. And it can be very, very small. But I like the last step, which is: be as courageous as you can. So, for me, I’m just, I’m taking in leads from Bitten. There are a lot of leads and I’m just following them through, just hoping that we can get to some of these documents that will release the information. What was released where? This is 50-years-old stuff, and it should be declassified. We have a problem with the declassification of everything in our government now, and we can’t hold them accountable for violating our freedoms if it isn’t transparent.
“We have a problem with the declassification of everything in our government now, and we can’t hold them accountable for violating our freedoms if it isn’t transparent.”
—Kris Newby
Kris Newby: I would say to everybody to try to do something small and to move the needle, it has to be the grassroots. Maybe get involved in Bonnie Crater’s Center for Lyme Action, which has done a lot to pretty much double the funding in the US government for the Lyme research. So that means getting on calls with your politicians, writing letters. It’s very easy to do that. Donate to people like ProPublica who are independent journalists that will speak truth to power. Help educate doctors from the ground up. So, I worked for this foundation for the last two and a half years, Invisible International, and they have free medical education courses for all the tick-borne diseases. They’re free. Watch them so you can be educated. Share them with your physicians so they can learn, so they learn more than their 15 minutes of medical school’s training on tick-borne diseases, or the propaganda coming from the infectious diseases people. So, ground up, help friends get to doctors who are experienced with Lyme disease. These are little things everyone can do.
Dana Parish: I love that. Thank you. Kris, where can we find your book? Where can we watch your movie? Under our Skin?
Kris Newby:
Bitten can be bought from Amazon or preferably your independent bookstores, or from HarperCollins, the publisher. There are audio and Kindle versions. I know a lot of Lyme people can’t read anymore. And then the film—it’s available online, just Google it. And it’s always changing who’s distributing it, but you can watch it on Freevee with ads for free or Vudu, I think is the video thing where you can watch it for $3.95 or from Under our Skin, the website. You can watch it through there, too.
Dana Parish: Great. And I highly recommend both your book and your film, both are extremely informative and give deep insight into what’s happening now with the Covid pandemic. There’s extreme overlap going on with these two diseases. Thank you so much for your insight today, Kris. I love talking to you. Anything I missed? Did I forget anything, or did we cover all the ground that we had hoped to?
Kris Newby: We could talk forever, but I just really appreciate that you’re helping on the Long Covid side too. Because the numbers are even bigger than for chronic Lyme, and patients are just so desperate for help and they don’t deserve the gaslighting they’re getting.
Dana Parish: It’s devastating. Well, thanks for saying that. I am doing my best to take your words to heart and do what I can. Play my small part in helping people get to the right answers, get to the truth, get to the right care. Thank you for all your support, and this has been amazingly fun for me. Thank you so, so much.
Kris Newby: Well, every day, get up. What can you do? That’s all you can do.
Note: You can find many of the documents referenced in this podcast and further information on Kris Newby’s website.
This blog is part of our BAL Spotlights Series. It is based on a transcript from Ticktective, our podcast and video series. To listen or watch the original conversation, please click here. Bay Area Lyme Foundation provides reliable, fact-based information so that prevention and the importance of early treatment are common knowledge. For more information about Bay Area Lyme, including our research and prevention programs, go to www.bayarealyme.org.
I was surprised that chronic fatigue syndrome was never mentioned since the government selected the name to block the name of myalgic encephalomyelitis. To try to silence those upset, they now use both names but shorten them by using merely the initials of ME and CFS.